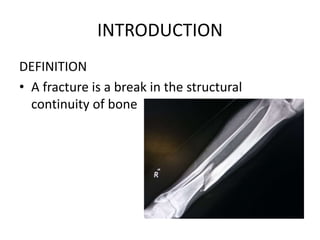
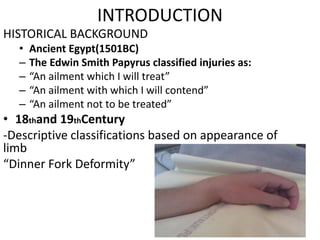
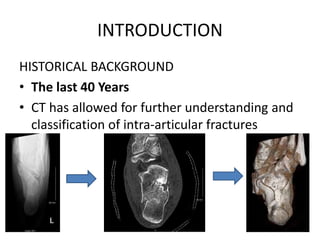
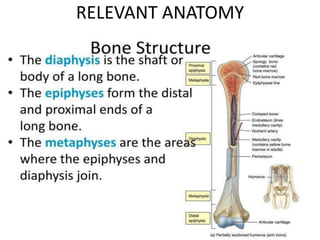
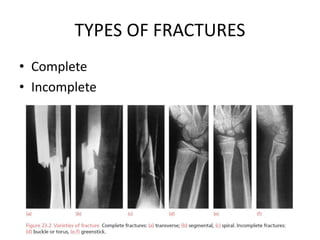
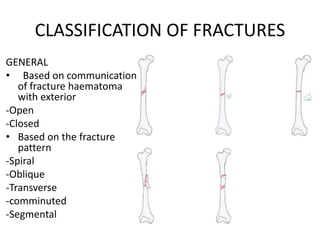
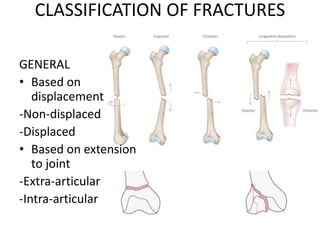
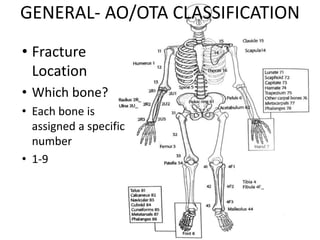
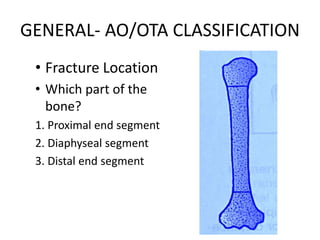
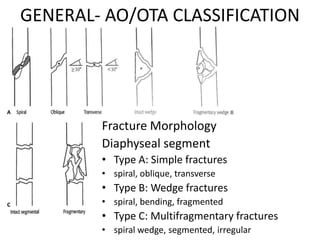
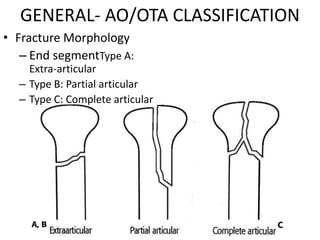
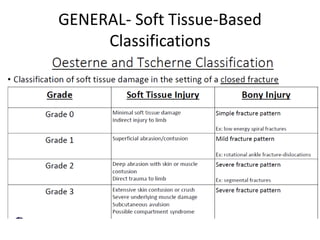
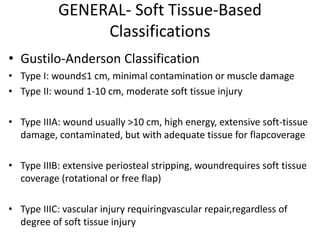
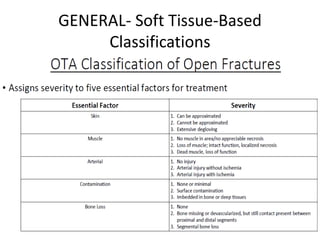
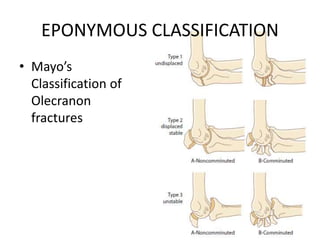
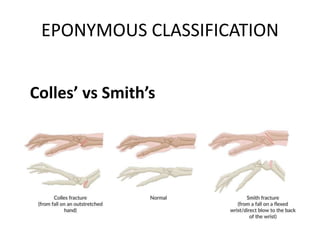
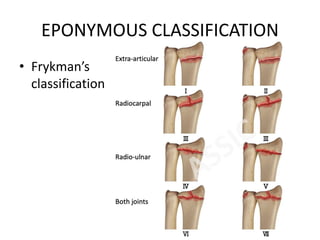
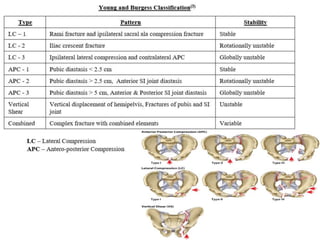
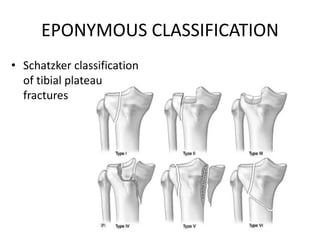
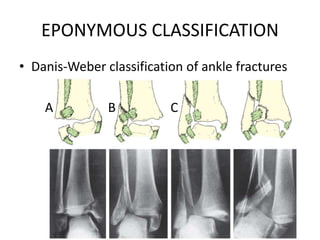
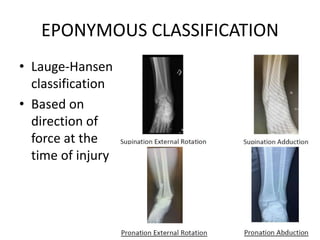
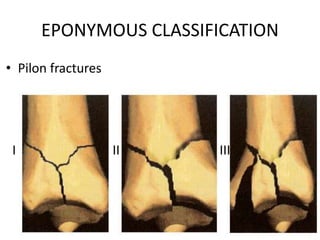
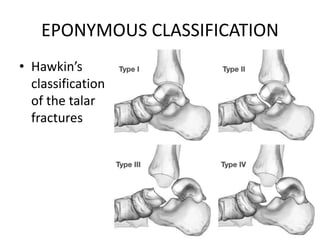
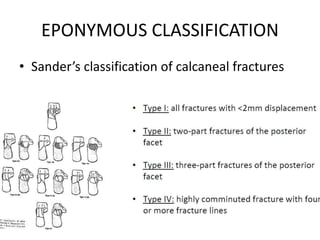
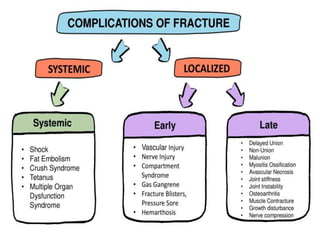
This document outlines the aetiology, classifications, and complications of fractures. It begins with definitions and historical background on fracture classifications. Key points include that fractures are caused by injury or repetitive stress and can be complete or incomplete. Several classification systems are described, including the AO/OTA system which categorizes fractures based on location and morphology. Eponymous classifications like Neer for proximal humerus fractures and Schatzker for tibial plateau fractures are also covered. Management depends on the classification and may involve operative or non-operative treatment. Classifications are important for communication, guidelines, and prognosis.