Total water daily requirement:
Depends upon age,size,temperature and body surface-
Most accurate guide is surface area 1.5 L/m2 area daily.
Practical guide is 30-40 ml/kg of total body weight Adult Male: 60%
Adult Female : 50% Infant:80%
Department of Surgery
NorthEast Medical College
Presentation on Fluid
and
Electrolytes Management
Presented By:
Dr. Nusrat Farhin Ahmed
&
Dr. Katha Acharjee
2.
Contents
● Total bodywater:
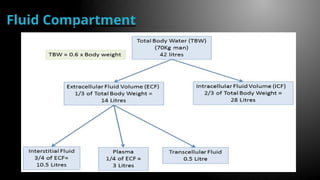
● Fluid Compartment
● Composition Of Fluid
Compartment
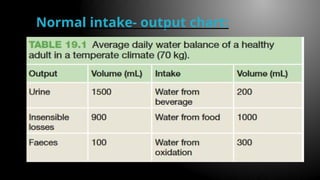
● Normal intake- output chart
● Disorder Of fluid Balance
● Assessment
● Monitoring Of fluid Balance
● Hypervolemia
3.
Total body water:
Totalwater daily requirement:
Depends upon age,size,temperature and body surface-
1.Most accurate guide is surface area 1.5 L/m2
area daily.
2.Practical guide is 30-40 ml/kg of total body
weight Adult Male: 60%
Adult Female : 50%
Infant:80%
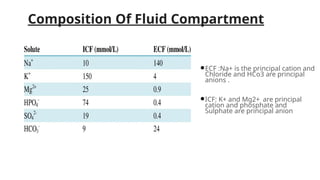
Composition Of FluidCompartment
●ECF :Na+ is the principal cation and
Chloride and HCo3 are principal
anions .
●ICF: K+ and Mg2+ are principal
cation and phosphate and
Sulphate are principal anion
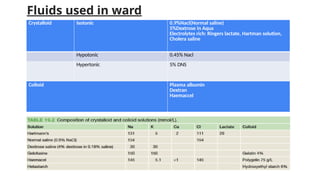
Fluids used inward
Crystalloid Isotonic 0.9%Nacl(Normal saline)
5%Dextrose in Aqua
Electrolytes rich: Ringers lactate, Hartman solution,
Cholera saline
Hypotonic 0.45% Nacl
Hypertonic 5% DNS
Colloid Plasma albumin
Dextran
Haemaccel
8.
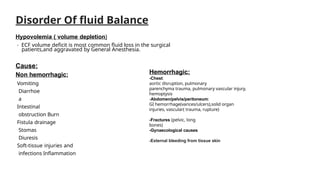
Disorder Of fluidBalance
Hypovolemia ( volume depletion)
- ECF volume deficit is most common fluid loss in the surgical
patients,and aggravated by General Anesthesia.
Cause:
Non hemorrhagic:
Vomiting
Diarrhoe
a
Intestinal
obstruction Burn
Fistula drainage
Stomas
Diuresis
Soft-tissue injuries and
infections Inflammation
Hemorrhagic:
-Chest:
aortic disruption, pulmonary
parenchyma trauma, pulmonary vascular injury,
hemoptysis
-Abdomen/pelvis/peritoneum:
GI hemorrhage(varices/ulcers),solid organ
injuries, vascular( trauma, rupture)
-Fractures (pelvic, long
bones)
-Gynaecological causes
-External bleeding from tissue skin
Sodium Balance
Distribution ofSodium
1. Total body sodium is 58 mmol/kg body weight
2. Distribution: ECF = 50%, ICF = 10%, Bone = 40%.
3. Exchangeable sodium is about 73%
14.
C/F:
Mild form patientis asymptomatic.
Na<120 mmol/L :patient become confused. There are sign-symptoms of water excess
1. Puffy face, JVP raised, High bounding pulse.
2.S/S of cerebral oedema like headache, vomiting, muscle twitching, poor co-ordination, then weakness,
apathy and confusion and finally coma and convulsion.
3. S/S of pulmonary oedema like cough, frothy sputum, basal crepitation
4. Low plasma Na. If plasma sodium falls below 110 mmol/L :Convulsion and coma may occur.
Hyponatraemia
15.
Measurement of Nadeficit in mmol
Total deficit = Body weight * (140-plasma
Na) * TBW in percentage
Sodium deficit if body weight is 60 kg and S
sodium is 130 mmol.
Total deficit = 60 X (140-130) X 60 /100 =
360 mmol.
16.
Treatment
1. Treatment ofunderlying cause.
2.Loss of Na can be replaced by sodium
intake or by giving I/V 0.9% saline.
3. Water retention should be treated by fluid
restriction.
17.
1. Clinical featuresare like that of water depletion.
2. Clinically patient is thirsty and drowsy.
3. Urine scanty with high specific gravity.
4. BP below normal
5. Serum sodium increased.
6. If serum Na rises above 160 mmol/L hypernatremic encephalopathy
Hypernatre
mia
Clinical
features
18.
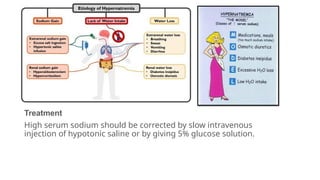
Treatment
High serum sodiumshould be corrected by slow intravenous
injection of hypotonic saline or by giving 5% glucose solution.
19.
Potassium Balance
Total bodypotassium is 3500 mmol/L or 50 mmol/kg body
weight.
ECF = 2%
ICF = 98%
Daily Requirement : 1 mmol/L
Control of Potassium balance by Aldosterone
20.
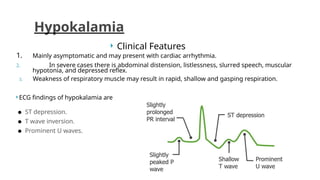
Clinical Features
1.Mainly asymptomatic and may present with cardiac arrhythmia.
2. In severe cases there is abdominal distension, listlessness, slurred speech, muscular
hypotonia, and depressed reflex.
3. Weakness of respiratory muscle may result in rapid, shallow and gasping respiration.
ECG findings of hypokalamia are
● ST depression.
● T wave inversion.
● Prominent U waves.
Hypokalamia
21.
Treatment of hypokalemia
Treatmentof hypokalemia usually focuses on loss control, replacement,
and loss prevention.
The first step is to make sure that the primary problem causing the
hypokalemia is dealt with i.e changing a diuretic.
The second step is to replace the missing potassium. For mild hypokalemia,
oral
supplements are often enough to replace the missing potassium. Potassium
levels
of less than 2.5 mEq/L usually are treated with intravenous potassium. This
could be anywhere from two to six doses of the medication.
Finally, you need to take steps to help the patient prevent potassium losses
in the
future. This may mean nutritional or medication education to ensure that
the loss doesn't occur again
22.
Hyperkalemia
Hyperkalemia, is anelevated level of potassium (K+) in the blood
serum. Normal potassium levels are between 3.5 and 5.0 mmol/L
(3.5 and 5.0 mEq/L) with levels above 5mmol/L defined as
hyperkalemia.
Clinical Features: Typically this results in no symptoms.
Occasionally when severe it results in palpitations, muscle pain, muscle
weakness, or numbness. An abnormal heart rate can occur which can
result in cardiac arrest and death. This is preceded by ECG Changes-a
peaked T wave, prolonged P-R interval and widens QRS complex and
small P wave.
23.
More serious symptomsof hyperkalemia
include slow heart rate and weak pulse.
The severity is divided into mild (5.5-5.9
mmol/L), moderate (6.0-6.4 mmol/L),
and severe (>6.5 mmol/L).
Common causes include kidney failure,
hypoaldosteronism, and
rhabdomyolysis. A
number of medications can also cause
high
blood potassium including
spironolactone,
NSAIDS, and angiotensin
converting enzyme inhibitors.
24.
Treatme
nt
1. Infuse intravenoushypertonic saline (50%) dextrose infusion together
with
insulin (1 unit of insulin per 2 gm of carbohydrate) to transport
potassium from extracellular to intracellular fluid.
2. Calcium gluconate, Sodium bicarbonate.
3. Ion exchange resin by oral or enema.







![ELECTROLYTES PRESENTATION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/electrolytespresentationautosaved-240707104734-15e2362d-thumbnail.jpg?width=640&height=640&fit=bounds)



![WILLIAM__FLUID_AND_ELECTROLYTE[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/williamfluidandelectrolyte1-230310182617-481b32fd-thumbnail.jpg?width=640&height=640&fit=bounds)













































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

