The document presents case studies of three infants with congenital lung malformations mimicking pneumothorax, detailing their clinical presentations, diagnostic workups, and treatments. It highlights the importance of recognizing congenital pulmonary malformations in young children presenting with respiratory distress and advocates for thorough evaluation and a multidisciplinary approach for effective management. Moreover, it discusses various types of congenital lung malformations and their histological features.











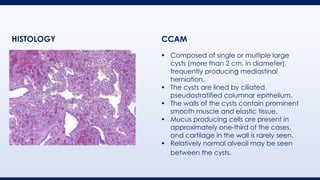
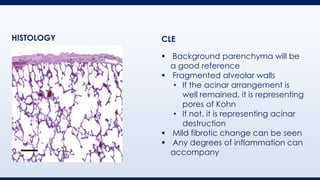














































![AIRWAY MALFORMATIONS AND FOREIGN BODIES [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/airwaymalformationsandforeignbodiesautosaved-250422152854-2cdd8e73-thumbnail.jpg?width=640&height=640&fit=bounds)





















