Downloaded 13 times




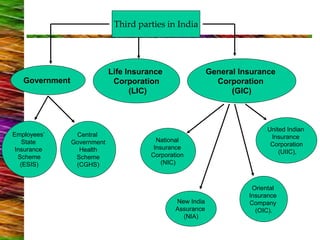


This document discusses healthcare systems and dental payment mechanisms in India and the United States. It provides details on: 1) The public and private healthcare sectors in India, including government insurance schemes like CGHS and ESIS. 2) Types of dental payment plans in the US, including private fee-for-service, insurance plans (HMOs, PPOs), and public programs like Medicaid and Medicare. 3) Reimbursement methods for dentists in the US, including UCR fees, fee schedules, and capitation. Major dental insurance plans like Delta Dental are also summarized.























































































