This document discusses various mechanisms for financing dental care, including:
- Private fee-for-service payments, where patients pay dentists directly.
- Third-party payment plans like insurance, which emerged to help cover rising healthcare costs. These include commercial insurance, nonprofit plans like Delta Dental, and public programs.
- Prepaid plans like HMOs, where dentists are salaried or contracted and patients pay fixed monthly fees for comprehensive care.
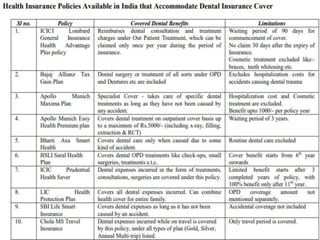
The history and types of third-party dental plans are described in detail. India primarily uses out-of-pocket fee-for-service payments due to low public spending on healthcare. Some early dental insurance plans in India are also mentioned.























![Tools of dental_public_health[1]](https://cdn.slidesharecdn.com/ss_thumbnails/toolsofdentalpublichealth1-151108134342-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






