Downloaded 101 times

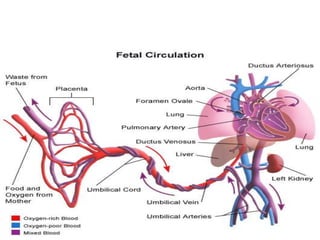
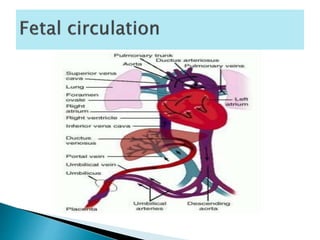
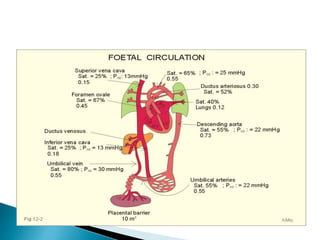




The document describes the fetal circulation and changes that occur at birth. In the fetus, oxygenated blood from the placenta travels to the heart and body while bypassing the lungs. At birth, the onset of breathing causes pulmonary vascular resistance to decrease and systemic resistance to increase. This results in blood shunting to the lungs, closure of the ductus arteriosus, and closure of the foramen ovale. The umbilical vessels also close, completing the transition to extrauterine life.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


