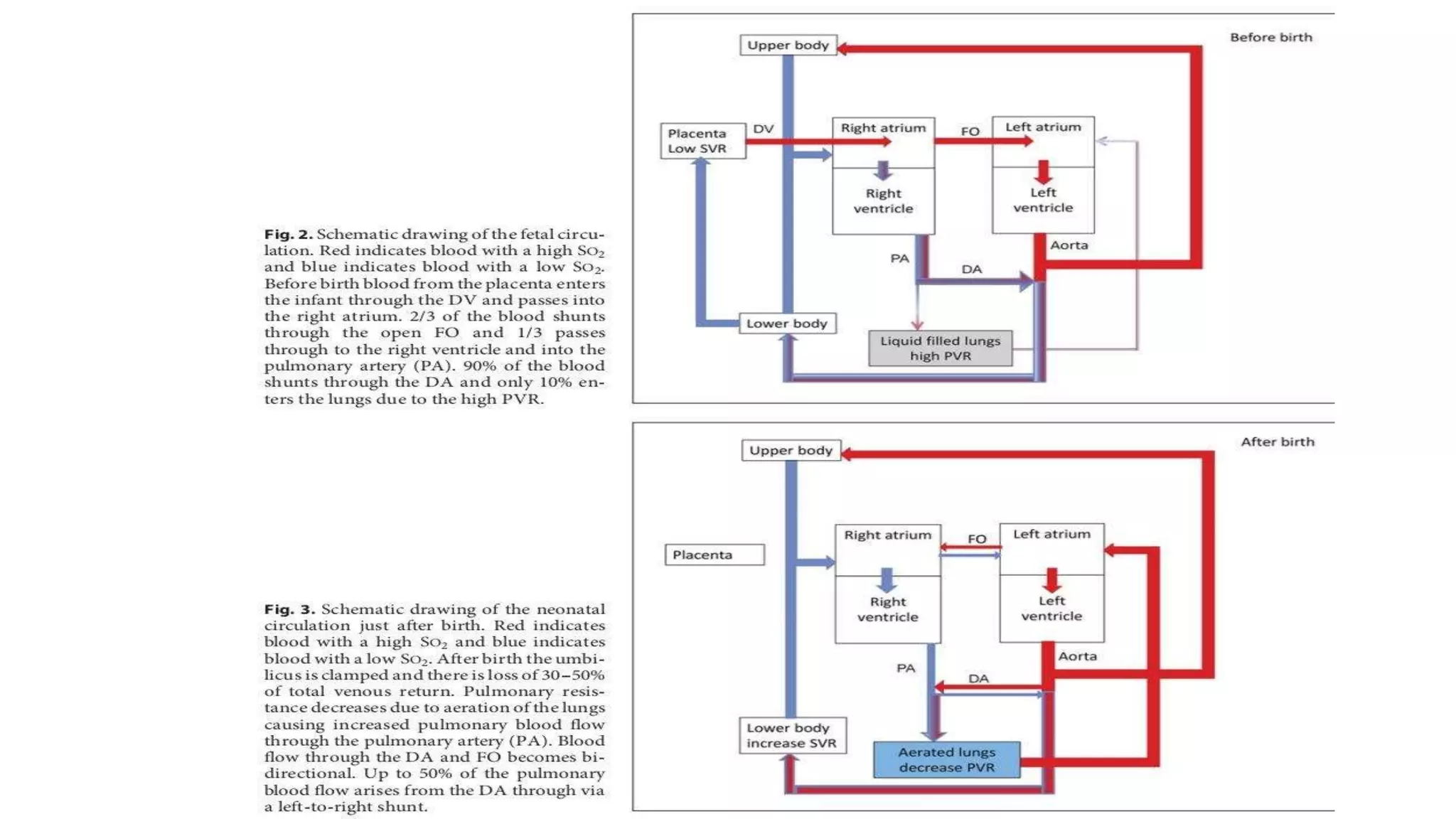
Fetal circulation differs significantly from adult circulation, with several shunts that allow blood to bypass the lungs and liver. At birth, major changes occur as the umbilical cord is clamped and the baby takes its first breath. The foramen ovale and ductus arteriosus close functionally immediately and anatomically over subsequent days. The ductus venosus becomes the ligamentum venosum. Failure of the shunts to close can result in congenital heart defects.