Pompili M. Fegato (Anatomia e Patologia Diffusa) Colecisti e Vie Biliari. ASM...Gianfranco Tammaro
PROF. POMPILI MAURIZIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
Indeterminate biliary strictures refer to biliary strictures without an identifiable cause on imaging. The endoscopist's role is to determine if the stricture is benign or malignant and offer treatment options. Available tools for evaluation include ERCP, cholangioscopy, intraductal ultrasound (IDUS), and endoscopic ultrasound (EUS). ERCP allows for tissue sampling but has limited sensitivity. Newer techniques like fluorescence in-situ hybridization and confocal endomicroscopy show promise to improve detection. Direct visualization with cholangioscopy may also improve detection over standard techniques. IDUS provides diagnostic accuracy without direct sampling. EUS allows for tissue acquisition with fine needle aspiration and evaluation of local
Pompili M. Fegato (Anatomia e Patologia Diffusa) Colecisti e Vie Biliari. ASM...Gianfranco Tammaro
PROF. POMPILI MAURIZIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
Indeterminate biliary strictures refer to biliary strictures without an identifiable cause on imaging. The endoscopist's role is to determine if the stricture is benign or malignant and offer treatment options. Available tools for evaluation include ERCP, cholangioscopy, intraductal ultrasound (IDUS), and endoscopic ultrasound (EUS). ERCP allows for tissue sampling but has limited sensitivity. Newer techniques like fluorescence in-situ hybridization and confocal endomicroscopy show promise to improve detection. Direct visualization with cholangioscopy may also improve detection over standard techniques. IDUS provides diagnostic accuracy without direct sampling. EUS allows for tissue acquisition with fine needle aspiration and evaluation of local
Caturelli E. Fegato Patologia Focale Benigna. ASMaD 2016Gianfranco Tammaro
DOTT. CATURELLI EUGENIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
O documento discute abdome agudo obstrutivo, com as principais causas sendo bridas, tumor de cólon, hérnias de parede abdominal e obstrução intestinal alta ou baixa. O diagnóstico é clínico com dor abdominal em cólica, náuseas, vômitos e parada de eliminação. Raios-X e TC de abdome podem ajudar na avaliação. Tratamento depende da presença de peritonite, podendo ser conservador ou cirúrgico.
This document discusses esophageal stents for malignant and benign indications. It describes the types of stents used, including plastic and metal stents. Complications include recurrent dysphagia, pain, hemorrhage and fistula formation. Stents are used for malignant strictures, benign strictures and ruptures/leaks. Fully covered metal stents are preferred for benign uses. New developments may include biodegradable stents and stents combined with radiation or antifibrotic drugs.
The document summarizes the evolution of bowel anastomosis techniques from the early 19th century to modern practices. It describes early techniques such as Glover's suture and Lembert's suture. Lembert introduced the concept of sero-serous sutures rather than muco-mucosal sutures. It also discusses modified techniques by Dupuytren, Jobert, Czerny, and Kocher. Modern techniques now use a double layer approach with synthetic absorbable sutures. Key considerations for a successful anastomosis include minimizing tension, ensuring blood supply is maintained, and allowing for physiological healing over 10-14 days.
Common Bile Duct Stones: Leave Them Get Them or Refer ThemGeorge S. Ferzli
The document discusses various approaches for managing common bile duct (CBD) stones, including:
- Preoperative identification using blood tests, ultrasound, ERCP, MRCP, which have varying sensitivity and specificity
- Intraoperative options like cholangiography, laparoscopic ultrasound, and indocyanine green injection
- Postoperative ERCP can be used for diagnostic and therapeutic purposes but has risks of pancreatitis and cholangitis
- The optimal management strategy depends on individual patient risk factors and circumstances.
- Laparoscopic repair of recurrent inguinal hernias has low recurrence rates of 0-1.1% and is associated with less pain and faster recovery compared to open repair.
- TEP repair is an effective procedure for treating direct, indirect, pantaloon, and recurrent hernias through small incisions with early return to normal activities and is a reliable technique for recurrent hernia repair after previous endoscopic herniorrhaphy.
- The learning curve for TEP is longer than for open repair, with some studies suggesting surgeons need to perform more than 100-250 laparoscopic procedures before recurrence rates fall below 5%.
Caturelli E. Fegato Patologia Focale Maligna. ASMaD 2016Gianfranco Tammaro
DOTT. CATURELLI EUGENIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
Why should I choose Laparoscopic Appendicectomy?
Should I remove a normal looking Appendix?
Should I always do an Interval Appendicectomy?
Tips and Tricks! How I Do It?
Dr. Mohamad Al-Gailani FRCS
Consultant Surgeon
Al Hammadi Hospital, Nuzha
Riyadh
Kingdom of Saudi Arabia
1) Aggressive fibromatosis is a rare soft tissue tumor that typically affects young adults. Surgery is the main treatment but recurrence is common.
2) New evidence shows systemic therapies like sorafenib, hormonal therapies, and chemotherapy can control the disease. A large trial found sorafenib significantly reduced recurrence compared to placebo.
3) Further research is still needed to determine optimal chemotherapy regimens and biomarkers to predict response to various treatments. "Wait and watch" may be suitable for less aggressive cases. Management of fibromatosis remains challenging due to the lack of high-quality data from India and validated patient-reported outcome measures.
Caturelli E. Fegato Patologia Focale Benigna. ASMaD 2016Gianfranco Tammaro
DOTT. CATURELLI EUGENIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
O documento discute abdome agudo obstrutivo, com as principais causas sendo bridas, tumor de cólon, hérnias de parede abdominal e obstrução intestinal alta ou baixa. O diagnóstico é clínico com dor abdominal em cólica, náuseas, vômitos e parada de eliminação. Raios-X e TC de abdome podem ajudar na avaliação. Tratamento depende da presença de peritonite, podendo ser conservador ou cirúrgico.
This document discusses esophageal stents for malignant and benign indications. It describes the types of stents used, including plastic and metal stents. Complications include recurrent dysphagia, pain, hemorrhage and fistula formation. Stents are used for malignant strictures, benign strictures and ruptures/leaks. Fully covered metal stents are preferred for benign uses. New developments may include biodegradable stents and stents combined with radiation or antifibrotic drugs.
The document summarizes the evolution of bowel anastomosis techniques from the early 19th century to modern practices. It describes early techniques such as Glover's suture and Lembert's suture. Lembert introduced the concept of sero-serous sutures rather than muco-mucosal sutures. It also discusses modified techniques by Dupuytren, Jobert, Czerny, and Kocher. Modern techniques now use a double layer approach with synthetic absorbable sutures. Key considerations for a successful anastomosis include minimizing tension, ensuring blood supply is maintained, and allowing for physiological healing over 10-14 days.
Common Bile Duct Stones: Leave Them Get Them or Refer ThemGeorge S. Ferzli
The document discusses various approaches for managing common bile duct (CBD) stones, including:
- Preoperative identification using blood tests, ultrasound, ERCP, MRCP, which have varying sensitivity and specificity
- Intraoperative options like cholangiography, laparoscopic ultrasound, and indocyanine green injection
- Postoperative ERCP can be used for diagnostic and therapeutic purposes but has risks of pancreatitis and cholangitis
- The optimal management strategy depends on individual patient risk factors and circumstances.
- Laparoscopic repair of recurrent inguinal hernias has low recurrence rates of 0-1.1% and is associated with less pain and faster recovery compared to open repair.
- TEP repair is an effective procedure for treating direct, indirect, pantaloon, and recurrent hernias through small incisions with early return to normal activities and is a reliable technique for recurrent hernia repair after previous endoscopic herniorrhaphy.
- The learning curve for TEP is longer than for open repair, with some studies suggesting surgeons need to perform more than 100-250 laparoscopic procedures before recurrence rates fall below 5%.
Caturelli E. Fegato Patologia Focale Maligna. ASMaD 2016Gianfranco Tammaro
DOTT. CATURELLI EUGENIO - Master ECM in Ecografia Internistica 2016 - Sabato 16 - 30 Gennaio e 13 Febbraio 2016 - Sala Congressi Fondazione Santa Lucia - Via Ardeatina n. 354 - ROMA
Sito ASMaD: http://www.asmad.net
Why should I choose Laparoscopic Appendicectomy?
Should I remove a normal looking Appendix?
Should I always do an Interval Appendicectomy?
Tips and Tricks! How I Do It?
Dr. Mohamad Al-Gailani FRCS
Consultant Surgeon
Al Hammadi Hospital, Nuzha
Riyadh
Kingdom of Saudi Arabia
1) Aggressive fibromatosis is a rare soft tissue tumor that typically affects young adults. Surgery is the main treatment but recurrence is common.
2) New evidence shows systemic therapies like sorafenib, hormonal therapies, and chemotherapy can control the disease. A large trial found sorafenib significantly reduced recurrence compared to placebo.
3) Further research is still needed to determine optimal chemotherapy regimens and biomarkers to predict response to various treatments. "Wait and watch" may be suitable for less aggressive cases. Management of fibromatosis remains challenging due to the lack of high-quality data from India and validated patient-reported outcome measures.
4LIFE INTERNATIONAL GROUP (www.4lifegroup.it ) nasce con l'intento di far conoscere a tutti un prodotto innovativo, il TRANSFER FACTOR, completamente naturale al 100%, frutto di 50 anni di ricerche e coperto con 4 brevetti mondiali, capace di informare e potenziare il nostro Sistema Immunitario affinchè il nostro organismo reagisca meglio alle più svariate malattie provocate da virus, neoplasie, allergie e malattie autoimmuni.
I Fattori di Trasferimento sono piccole molecole messaggere che trasferiscono informazioni immunologiche da un’entità ad un’altra, per esempio dalla madre al neonato. Le cause dell’indebolimento del nostro sistema immunitario sono molteplici e spesso legate allo stress, all’inquinamento e contaminazione ambientale, alla cattiva alimentazione, ai nuovi ceppi di “superbatteri” dovuto all’eccessivo consumo di medicine.
Anche gli antibiotici, usati troppo spesso e in dosi eccessive per combattere le infezioni hanno, a lungo termine, effetti negativi sul sistema immunitario
Le conseguenze di un sistema immunitario indebolito o deficitario, sono la causa di infezioni e malattie sempre più frequenti e prolungate.
I processi di estrazione dei Fattori di Trasferimento dal colostro vaccino e dal tuorlo dell’uovo, sono protetti da brevetto degli USA nr. 6.468.534 (colostro e tuorlo) e nr. 6.866.868 (tecnica di estrazione), ed altri brevetti in attesa di registrazione.
Oltre 3.000 ricerche scientifiche e test fatti in laboratori indipendenti, indicano che la formula 4Life Transfer Tri-Factor aumenta l’efficacia del sistema immunitario incrementando l’attività funzionale delle NK Cells (Cellule Natura Killer) del 473%.
Le cellule NK sono le barriere difensive del sistema immunitario.
The document discusses various cardiac conditions including:
1) Acute rheumatic fever which can cause small, firmly attached vegetations on heart valves that rarely cause problems and usually resolve after the acute episode.
2) Long-term effects of rheumatic fever include diffuse fibrosis and thickening of heart valves, sometimes with calcification, resulting in stenosis.
3) Images show marked mitral valve stenosis and calcification as well as less severe tricuspid valve involvement from rheumatic fever. The mitral and aortic valves are more commonly affected than the tricuspid or pulmonary valves.
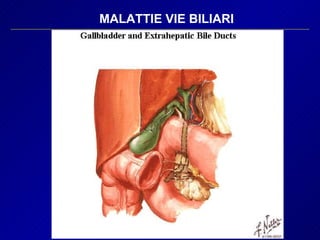
16. MALATTIE VIE BILIARI - CALCOLOSI COLECISTI, COLEDOCO E COMPLICANZE - TUMORI - MALFORMAZIONI V.B. E DUODENO, DIVERTICOLI - ESITI PANCREATITE - LESIONI IATROGENE
17. Calcolosi Circa 10% USA Calcoli: - colesterinici puri: rari - 30% bilirubinato di Calcio con 30% di Colesterolo - 70% MISTI colesterolo 70%, sali di calcio, sali biliari, proteine Decorso Clinico - Asintomatico 80% di cui 15% Sintomatico entro 10 aa. - Sintomatico 20% di cui 35% Complicato “ “ “ “
24. Colecistite Acuta SINTOMATOLOGIA 1-a Dolore per contrazione parossistica della colecisti Inizialmente a prevalente carattere accessionale tipico della colica biliare e successivamente continuo per il progressivo interessamento della sierosa della colecisti Precedenti Episodi (60%) Assenza di Episodi (40%) Viscerale profondo, mal localizzabile (solitamente il paziente lo riferisce ad insorgenza epigastrica)
25. Colecistite Acuta SINTOMATOLOGIA 1-b Successiva irradiazione in ipocondrio destro Irradazione al dorso, in sede sottoscapolare dx, spalla dx, e base del collo a dx (coinvolgimento del nervo frenico ), caudalmente al fianco dx Interessamento dei quadranti addominali limitrofi: progressione della flogosi verso i visceri circostanti con formazione di aderenze dapprima lasse e poi tenaci Irradiazione verso ipocondrio sx: Edema pancreatico concomitante Nausea e Vomito (70%) dapprima alimentare poi biliare Iperpiressia (80%)
26. Colecistite Acuta Punti dolorosi nelle affezioni epatobiliari: 1- Punto cistico 2- Punto costale 3- Zona Coledocopancreatica di Chauffard Rivet
27. Colecistite Acuta Punti frenici: La compressione di questi punti può risultare dolorosa non solamente nelle pleuriti diaframmatiche, ma anche in tutte le flogosi addominali con interessamento del diaframma (es. Colecistite)
28. Colecistite Acuta ESAME OBIETTIVO Contrazione di difesa nei quadranti addominali superiori, prevalentemente in ipocondrio dx Segno di Murphy positivo , talvolta spontaneo con limitazione antalgica delle escursioni respiratorie In molti casi la colecisti, distesa è agevolmente palpabile in ipocondrio destro Talvolta si associa subittero o ittero per iperplasia dei linfonodi pericoledocici che ostacolano il deflusso biliare e/o ipertono oddiano secondario ( nel 10%dei casi si associa Calcolosi del Coledoco) Il quadro conclamato della colecistite può non essere apprezzabile nei diabetici, anziani, pazienti nel post-operatorio
29.
30.
31.
32.
33. Colecistite Acuta PROGRESSIONE del PROCESSO INFIAMMATORIO dal SUO ESORDIO Da necrosi ischemica alla possibile perforazione e peritonite biliare ACME Rapida Progressione Regressione dell’edema e delle emorragie intramurali e comparsa di elementi fibroblastici propri dell’evoluzione cicatriziale del processo finché in media dalla 5° settimana compare la componente granulomatosa configurante il quadro della colecistite sclero-atrofica DECORSO Possibile coinvolgimento secondario dello Sfintere di Oddi compatibile con esito in papillite
75. ITTERO OSTRUTTIVO CONSEGUENZE FUNZIONALI DELLA COLESTASI Sali Biliari Ridotta concentrazione intestinale Ritenzione a livello sistemico Aumento a livello sistemico Diminuito arrivo nell’intestino Bilirubina Malassorbimento lipidi, vitamine Steatorrea Malnutrizione Osteodistrofia S. Emorragica Effetto irritante terminazioni neurosensoriali Prurito Aumentata filtrazione glomerulare Accumulo nella cute Acolia fecale Disfunzione tubulare renale Ittero
76.
77. ITTERO OSTRUTTIVO CAUSE DI COLESTASI EXTRAEPATICA 1-a Calcolosi Tumori Benigni : Adenomi, papillomi, cistoadenomi, Fibromi Maligni : Colangiocarcinoma T. Papilla di Vater: AdenoCr, Sarcoma, Carcinoide, Provenienza Duodeno Processi che comportano compressione estrinseca Carcinoma testa pancreas Pseudocisti pancreatica Pancreatite Acuta e Cronica Tumefazioni di Linfonodi ilari o pericoledocici Peritonite Adesiva da perforazione ulcera duodenale Diverticolo Duodenale periampollare
78. ITTERO OSTRUTTIVO CAUSE DI COLESTASI EXTRAEPATICA 2-a Processi Flogistici Stenosi benigna Post-chirurgica Trauma Addominale Ulcera duodenale perforata o penetrante Pancreatite Cronica Varie Cisti Coledociche, Ascessi Amebici, Infezioni Parassitarie, Emobilia, Discinesia dei dotti biliari e dello sfintere di Oddi
79. ITTERO OSTRUTTIVO SINTOMI E SEGNI ITTERO in genere ingravescente con iperbilirubinemia a prevalente quota diretta PRURITO che può precedere o essere associato all’ittero URINE SCURE per bilirubinuria FECI IPO-ACOLICHE Es. EMATOCHIMICI Fosfatasi Alcalina Gammaglutamiltranspeptidasi Acidi Biliari Sierici