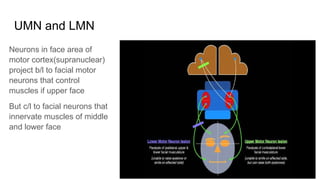
UMN and LMN
Neuronsin face area of
motor cortex(supranuclear)
project b/l to facial motor
neurons that control
muscles if upper face
But c/l to facial neurons that
innervate muscles of middle
and lower face
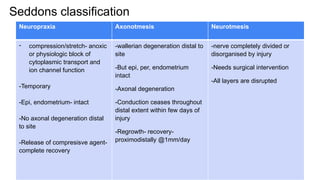
Seddons classification
Neuropraxia AxonotmesisNeurotmesis
- compression/stretch- anoxic
or physiologic block of
cytoplasmic transport and
ion channel function
-Temporary
-Epi, endometrium- intact
-No axonal degeneration distal
to site
-Release of compresisve agent-
complete recovery
-wallerian degeneration distal to
site
-But epi, per, endometrium
intact
-Axonal degeneration
-Conduction ceases throughout
distal extent within few days of
injury
-Regrowth- recovery-
proximodistally @1mm/day
-nerve completely divided or
disorganised by injury
-Needs surgical intervention
-All layers are disrupted
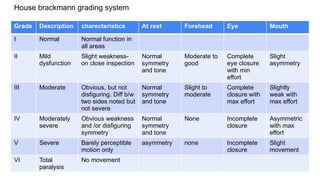
House brackmann gradingsystem
Grade Description charecteristics At rest Forehead Eye Mouth
I Normal Normal function in
all areas
II Mild
dysfunction
Slight weakness-
on close inspection
Normal
symmetry
and tone
Moderate to
good
Complete
eye closure
with min
effort
Slight
asymmetry
III Moderate Obvious, but not
disfiguring. Diff b/w
two sides noted but
not severe
Normal
symmetry
and tone
Slight to
moderate
Complete
closure with
max effort
Slightly
weak with
max effort
IV Moderately
severe
Obvious weakness
and /or disfiguring
symmetry
Normal
symmetry
and tone
None Incomplete
closure
Asymmetric
with max
effort
V Severe Barely perceptible
motion only
asymmetry none Incomplete
closure
Slight
movement
VI Total
paralysis
No movement
9.
Altered function offacial nerve after injury
● Distance between nodes of ranvier is altered
● Newly formed axons are covered with myelin that is much thinner than normal
axon
● Splitting and crossing of axons that reinnervate the denervated muscle groups
without cell body motor unit arrangement
Tics or involuntary twitching occurs-
Movement of mouth with blinking /closing of eye with smiling
Hyperkinesis- ephaptic transmission – depolarization at site of injury acts as
stimulus to intact portion of fibre capable of exciting adjacent fibres in the area
10.
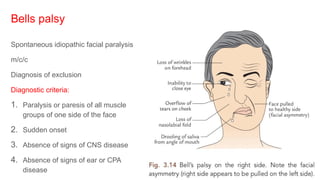
Bells palsy
Spontaneous idiopathicfacial paralysis
m/c/c
Diagnosis of exclusion
Diagnostic criteria:
1. Paralysis or paresis of all muscle
groups of one side of the face
2. Sudden onset
3. Absence of signs of CNS disease
4. Absence of signs of ear or CPA
disease
11.
● Proposed etiology:
-Microcirculatory failure of the vasa nervorum
- Viral infection
- Autoimmune reactions
- Viral hypothesis- highly accepted- mumps, rubella, HSV,EBV, VZV
Temporary
Permanent recovery within 3months occur in 90% pts
12.
● Sudden onset
●Unable to close eye
● Bells phenomeon- eyeball rolls up and out on attempting to close the eye and
white sclera is visible
● Facial asymmetry
● Deviation of mouth
● Dribbling of saliva
● Loss of taste
● Epiphora
13.
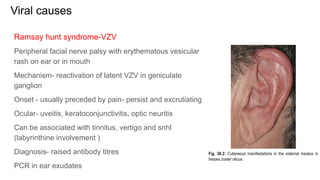
Viral causes
Ramsay huntsyndrome-VZV
Peripheral facial nerve palsy with erythematous vesicular
rash on ear or in mouth
Mechanism- reactivation of latent VZV in geniculate
ganglion
Onset - usually preceded by pain- persist and excrutiating
Ocular- uveitis, keratoconjunctivitis, optic neuritis
Can be associated with tinnitus, vertigo and snhl
(labyrinthine involvement )
Diagnosis- raised antibody titres
PCR in ear exudates
14.
Prognosis is worsethan bells
Persistent weakness- 30-50%, only 10%- complete recovery
Steroid + antiviral
Prednisone -1mg/kg/day for 5 days f/b tapered in 10days
Acyclovir - 800mg fivetimes daily
15.
EBV-
● Generalised lymphadenopathy
●Fever
● Throat pain
● Facial nerve palsy (B/L)
● Diagnosis- 10% atypical lymphocytes and positive serology
HIV- facial pasly can present at any stage of the disease
● Possible mechanism-
● local infection of facial nerve or geniculate ganglion by HIV
● inflammatory demyelinating neuropathy or
● secondary infection with VZV,HSV or EBV due to immunosuppression
16.
GB Syndrome
Acute inflammatorydemyelinating polyradiculoneuropathy affecting peripheral nerves
including facial nerve
Presents typically 2-3weeks after an urti- probably due to abnormal T-cell response against
Most prominent – ascending symmetrical muscular weakness and autonomic involvement
with maximum effect 2-3weeks after onset of illness
Often b/l facial nerve weakness
Treatment- IVIg
17.
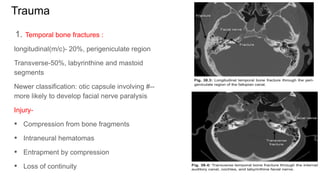
Trauma
1. Temporal bonefractures :
longitudinal(m/c)- 20%, perigeniculate region
Transverse-50%, labyrinthine and mastoid
segments
Newer classification: otic capsule involving #--
more likely to develop facial nerve paralysis
Injury-
• Compression from bone fragments
• Intraneural hematomas
• Entrapment by compression
• Loss of continuity
18.
● Penetrating injuries/gun shot :
• Often accompanied with severe dural tears, csf leak, damage to otic capsule
and vascular injury
• m/c- mastoid segment
• Surgical exploration – as soon as possible
• Delay- make identification of nerve difficult- granulation tissue and traumatic
neuroma formation
• If segment of nerve is destroyed- proximal and distal ends- trimmed back- to
point of healthy fascicles – interval cable graft
19.
Iatrogenic
• Cautery heattrauma
• Plication or suspension sutures entrapping a branch of nerve
• Inadvertent clamping of nerve when ligating vessels
• Postop edema- nerve compression
20.
ME and mastoidsurgery:
• m/c site- distal tympanic segment and 2nd
genu> mastoid segment
• If recognized intraop- exploration with decompression of prox and distal
segments
• If nerve fibres- herniating-> epineural sheath should be opened
• If >50% of circumference is disrupted- repaired- direct suture or inlay graft
21.
If observed immediatepostop-
• Determine – nerve was identified and was not at risk during surgery-
observation for few hours- clear local anesthetic induced weakness
• Tight mastoid dressing- remove the pack
• If paralysis is incomplete- start on oral steroids and observe clinically
• Progression to complete paralysis- exploration should be considered
22.
Parotid surgery:
• Likelihoodof facial nerve weakness correlates with-
• Tumor location deep to plane of facial nerve
• Previous parotid surgery
• Previous sialadenitis
Parotid surgery- best undertaken with facial nerve monitoring
If no response- nerve and its branches could be closely inspected for areas of
discontinuity
23.
As a complicationof ear infection
Otitis media:
• Direct involvement of facial nerve by infection through facial canal dehiscence
or physiologic canaliculi for neurovascular connections
• Fallopian canal osteitis with bone erosion
• Inflammatory edema – compression
• secondary thrombosis of vasa nervorum- ischemia and infarction of facial nerve
• Demyelination of facial nerve by bacterial toxins
24.
MOE:
• Immunocompromised ,DM
• Facial palsy - advancing infection and invasion through bonycartilaginous
junction and fissures of Santorini , under the tympanic ring and posteriorly to
SMF
25.
Inflammatory disorders
Sarcoidosis :facial palsy, heerfordt disease, raised ACE titre
Granulomatosis with polyangitis : autoimmune necrotizing vasculitis
secondary to middle ear involvement in presence of dehiscent fallopian canal
Snhl+ facial palsy+ urti+ kidney vasculitis
Diagnosis- ANCA
Lyme disease- flu like symptoms, erythema migrans
b/l facial palsy
26.
Congenital
• Melkerson Rosenthalsyndrome – facial palsy, facial edema, fissured tongue
• Moebius syndrome- agenesis of 6,7 CN nuclei , mask like face, unable to
close eyes
• Alberg Schoenberg disease- osteopetrosis of bony canals- blindness,
deafness and facial paralysis.
• Oculoauricular –vertebral syndrome- abnormal formation of 1 and 2nd
arches
• Charge association
27.
Transient facial palsy
•During IAN block
• Due to injection of local anesthetic into parotid - needle injected too backwards
• Temporary
• Wears off within a period of time
Other causes:
• Barotrauma
• Pregnancy
• Malignancies
• Benign tumors- schwannoma, glomus
28.
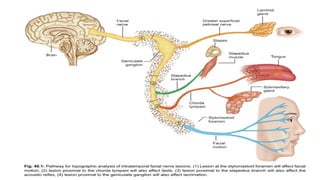
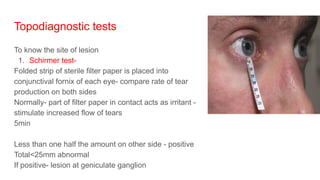
Topodiagnostic tests
To knowthe site of lesion
1. Schirmer test-
Folded strip of sterile filter paper is placed into
conjunctival fornix of each eye- compare rate of tear
production on both sides
Normally- part of filter paper in contact acts as irritant -
stimulate increased flow of tears
5min
Less than one half the amount on other side - positive
Total<25mm abnormal
If positive- lesion at geniculate ganglion
29.
2. Stapedius reflex
Involuntarymuscle contraction in response to high intensity sound stimulus
Absent reflex or reflex less than one half the amplitude on contralateral side is
abnormal
3. Taste
Filter paper disks impregnated with aqueous solutions of
NaCl- salty
Sachharose-sweet
Citrate or hydrochloric acid - sour taste
Quinine- bitter
Or by electrogustometry - bipolar or monopolar electrical stimulation - metallic or
sour taste
30.
4. Salivary flowtest - evaluates parasympathetic innervation of SMG via chords
tympani
Cannulation of SM DUCT- comparison of stimulated flow rates on both sides
using radiolabelled tracer secreted in saliva
25% decrease- significant
5. Salivary pH
<6.1 - incomplete recovery in bells palsy
31.
Electrodiagnostic tests
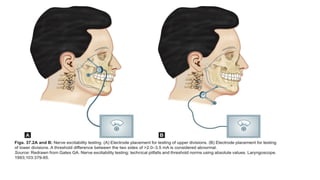
1. Nerveexcitability test
Stimulating electrode- skin over SMF or over one of peripheral branches of nerve
Return electrode- taped to forearm
Electrical impulses(0.3sec ) -steadily increasing current levels- until facial twitch is
noted (Threshold of excitation)
Same repeated on paralysed side
Diff is calculated
Sunderland-1 - no diff
2-5-- axonal degeneration- diff present
2-3.5mA diif - sign of severe degeneration - indicator for surgical decompression
33.
Maximum stimulation test
•Involves visual /subjective evaluation of electrically elicited facial movements
• Maximal stimuli - current level at which greatest amplitude of facial movement
is seen
• Supramaximal stimuli are noted
• Paralysed side is compared with normal- equal, mildly decreased, moderately
decreased or without response
• No response at maximal stimulation- criteria for facial nerve decompression.
34.
Electroneuronography
• 1 bipolarstimulationg electrode- SMF
• 2nd
bipolar electrode pair -in nasolabial groove
• Evoked responses to maximal electrical stimulation are measured as evoked
compound muscle action potential
• The amplitude of response on the paralyzed side can be expressed as a precise
percentage of that on the healthy side.
• if the amplitude of the response on the paralyzed side is only 10% of that on the
normal side-- an estimated 90% of fibers are said to have degenerated on the
paralyzed side.
35.
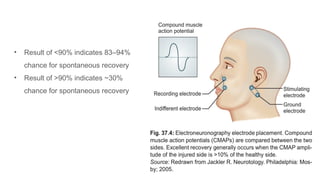
• Result of<90% indicates 83–94%
chance for spontaneous recovery
• Result of >90% indicates ~30%
chance for spontaneous recovery
36.
Electromyography
• Recording spontaneousand voluntary muscle potentials using needles
introduced into muscles
• After loss of excitability- NET and ENoG are not useful
• After 10-14 days – fibrillation potentials may be detected- confirms presence of
degenerating motor units incomplete recovery
• Polyphasic synaptic potentials- 4-6weeks after onset- indicate reinnervation –
good recovery
38.
Medical
1. Eye care
-Artificialtears (methylcellulose drops) every 1–2 hour and 4–5 times per day.
-Eye ointment followed by patching or taping the eye.
- Cover for the eye in night.
-Protect the eye from wind, foreign bodies and drying with glasses and moisture
chambers.
-Temporary tarsorrhaphy may be needed in some cases
2. Steroids – anti-inflammatory effect on neural edema
3. Antiviral therapy
4. Antibiotics
5. Analgesics
6. Physiotherapy
39.
Timing
Acute neural injury-wallerian degeneration – over 72hrs
• Starts at point of injury – extends distally to motor end plate of facial muscle
and proximally to first adjacent node of ranvier
• Electrodiag test- cant appreciate – underdiagnosis
• Once degeneration is complete- ENoG- helpful- day3-21- to quantify degree
of nerve degeneration
• By 21days- cell body and proximal segment reorganize
Retain ability to regenerate for indefinite period of time
Here EMG is helpful
40.
• Subacute neuralinjury- early regeneration phase- 3wks to 6mnths
• Possibility of recovery is more
• If no signs of any recovery within 3-4 wks – neurotmesis
• Chronic neural injury- no recovery within 6mnths of injury
Assess :
• Nerve continuity
• Viability of cell bodies in facial nucleus
• Presence of intact proximal facial segment
• Presence of distal segment with intact endoneural tubules- that can accept and
transmit regenerating axons to facial muscles
• Presence of viable facial muscles with intact motor end plates
• If fulfilling all above- spontaneous regeneration
• But –ocular and physio- to minimize aberrant regeneration
41.
Surgical
- Surgical decompression
-Neurorraphy- end to end anastomosis
- Nerve grafting – if there is gap between prox and distal segments- autogenous nerve
grafting
- Nerves- Hypoglossal nerve(crossover grafting)
- Sural nerve
- Greater auricular nerve
- Branches from cervical plexus
-Muscle transposition
-Tarsorrhaphy
-Gold/platinum lid weights