Downloaded 120 times


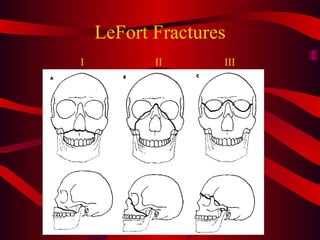

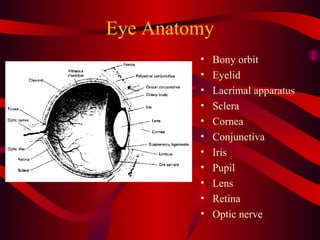

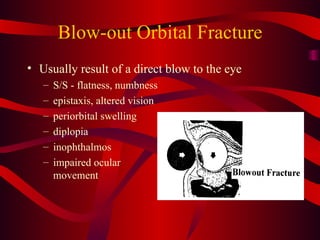


This document discusses various types of maxillofacial, ophthalmic, dental, and neck trauma. It covers the anatomy and physiology of these areas, common injuries including fractures, lacerations, and foreign bodies. Management priorities include airway control, bleeding control, spinal motion restriction, and rapid transport to a trauma center. Facial fractures include mandibular, maxillary, and LeFort patterns. Eye injuries require careful examination and irrigation. Dental trauma emphasizes finding and stabilizing avulsed teeth. Neck trauma zones and signs of vascular or airway injury are outlined.










































































































