Downloaded 36 times


































![[abducens, trochlear, om nucleus]
[cerebellum, brainstem]
[pprf, mrf]
[dorsal raphe]](https://image.slidesharecdn.com/eyemovements-161130184526/85/Eye-movements-35-320.jpg)


























































![• Square wave jerks (SW]) consist of
consecutive to-and-fro, horizontal saccades of
small amplitude (O.S-3"), with a 200-ms inter
saccadic interval.
• They usually increase during smooth pursuit
and fixation. SW} are found in cerebellar
pathology, degenerative diseases, particularly
in PSP, and, rarely, in hemispheric diseases.
•](https://image.slidesharecdn.com/eyemovements-161130184526/85/Eye-movements-94-320.jpg)
























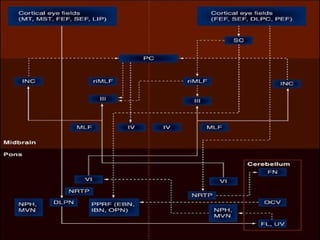




Eye movements serve to bring images onto the high-resolution fovea and increase visual range. There are five types of eye movements: saccades rapidly shift gaze; smooth pursuit tracks moving objects; vergence aligns eyes for near/far vision; vestibular-ocular reflex stabilizes gaze during head movements; and optokinetic reflex assists with slow eye movements. These movements are controlled by neural circuits involving the extraocular muscles, brainstem, cerebellum and cortex. Abnormalities in eye movements can provide clinical clues regarding underlying neurological disorders.



































































