Downloaded 26 times




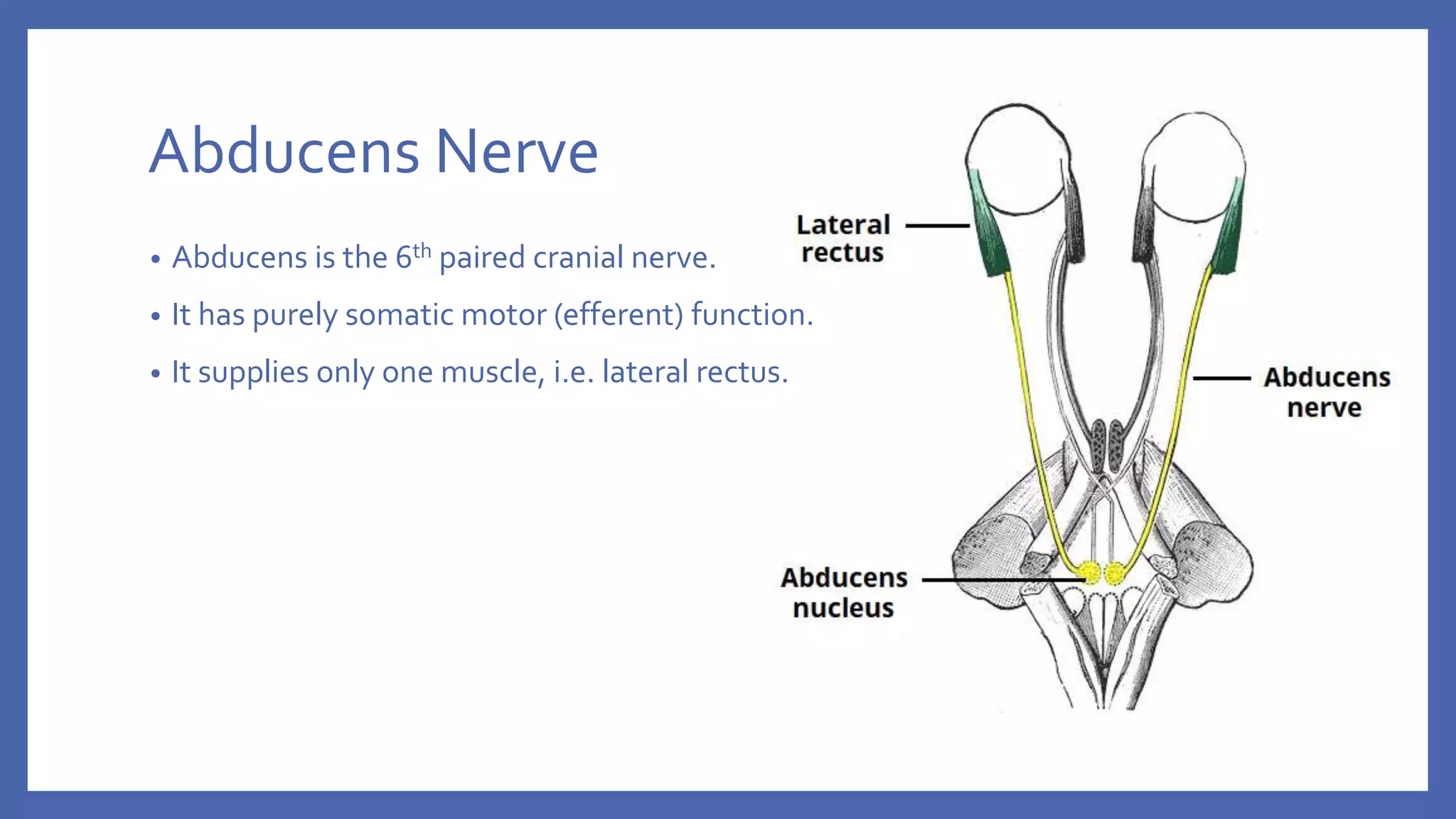
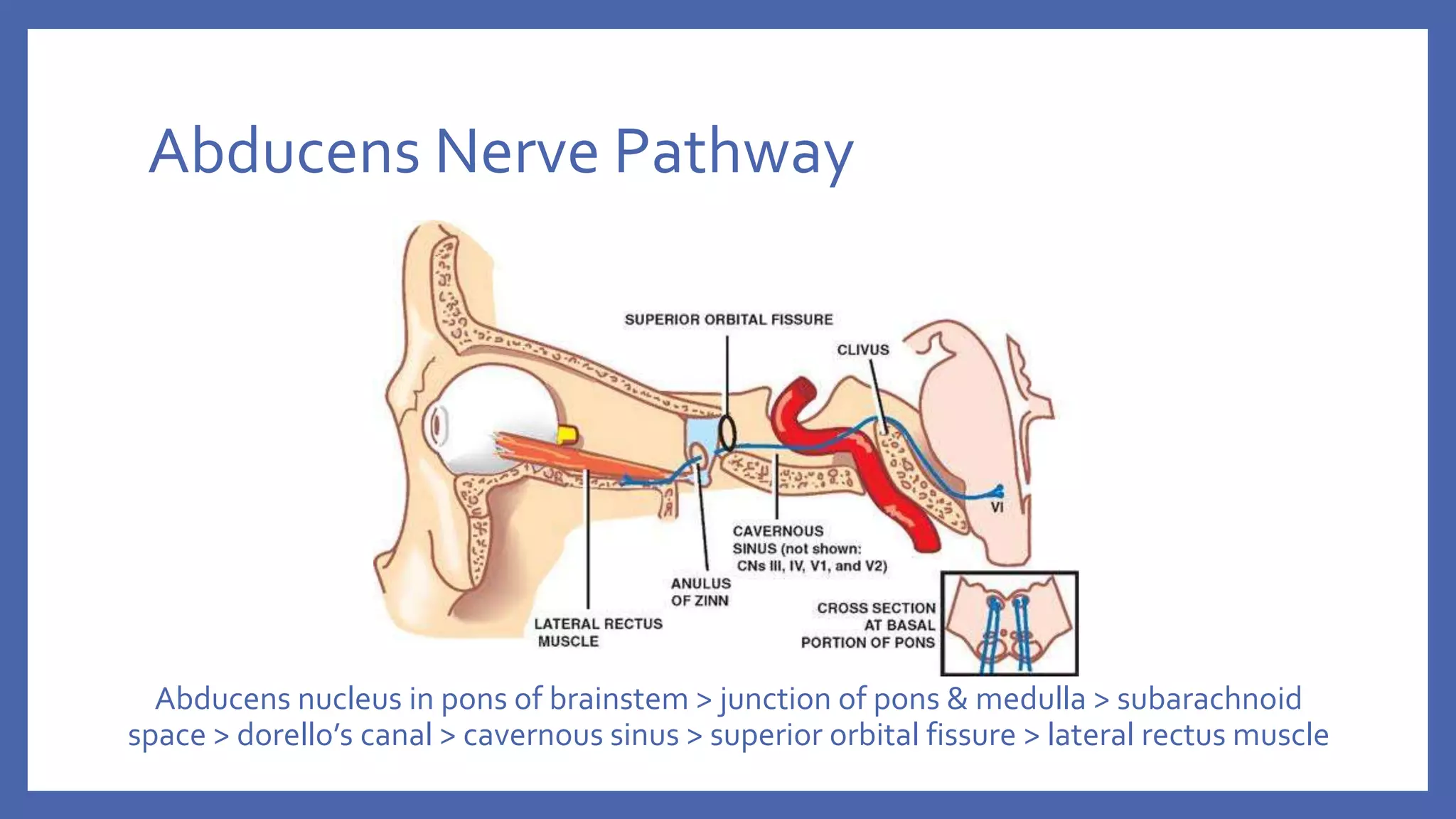















The document discusses the anatomy and function of the lateral rectus muscle and the 6th cranial nerve (abducens nerve), which controls eye abduction. It details the etiology, clinical features, differential diagnoses, and management strategies for 6th nerve palsy, both in unilateral and bilateral cases. Treatment options include conservative approaches for symptom relief and surgical interventions once the condition stabilizes.



































































