1. Major causes of external hemorrhage include penetrating trauma from high-velocity weapons, stab wounds, and blunt trauma, especially in young males.
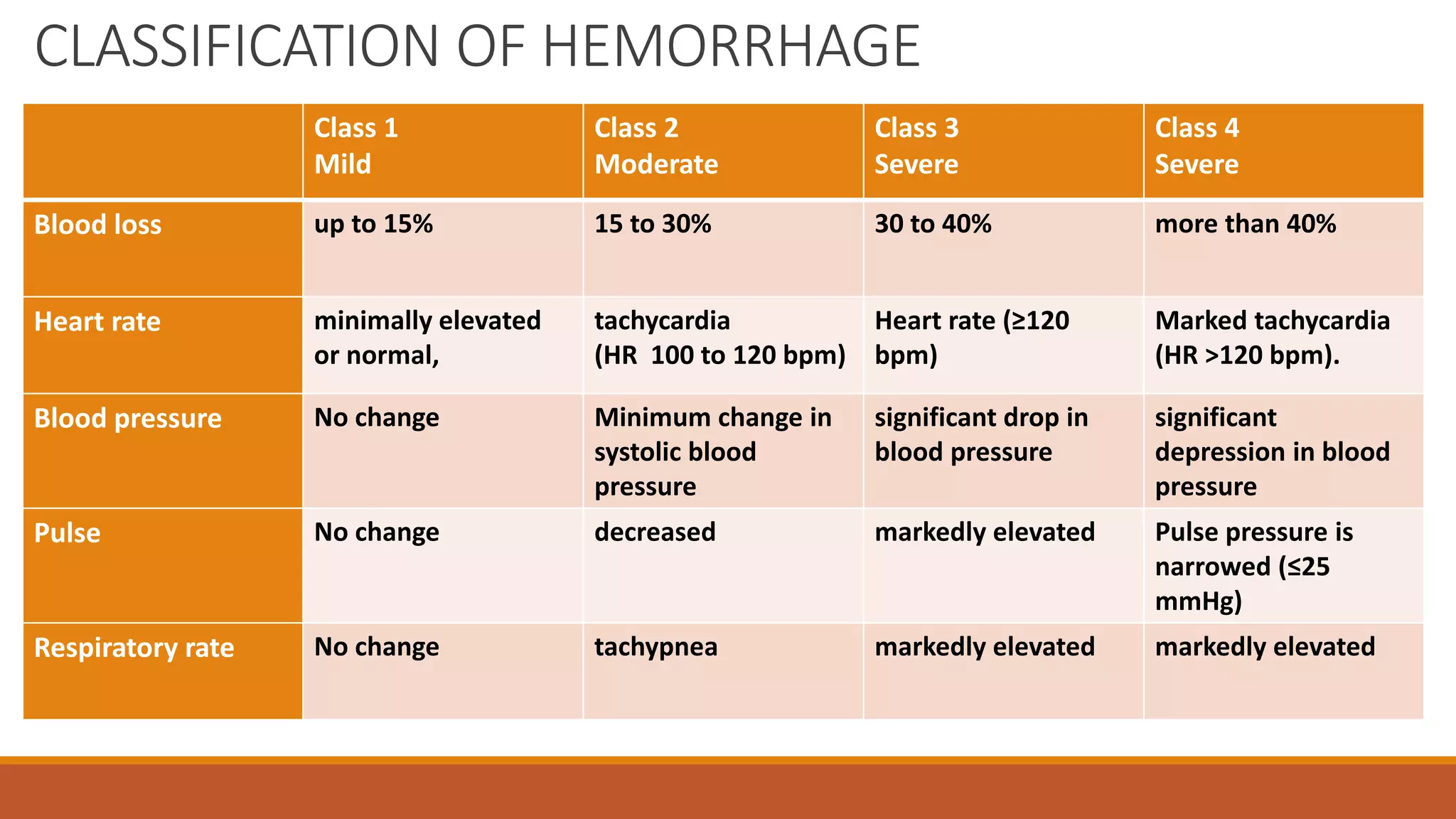
2. External hemorrhage is classified based on the degree of blood loss and physiological symptoms, ranging from mild with minimal changes to severe with more than 40% blood loss and marked physiological depression.
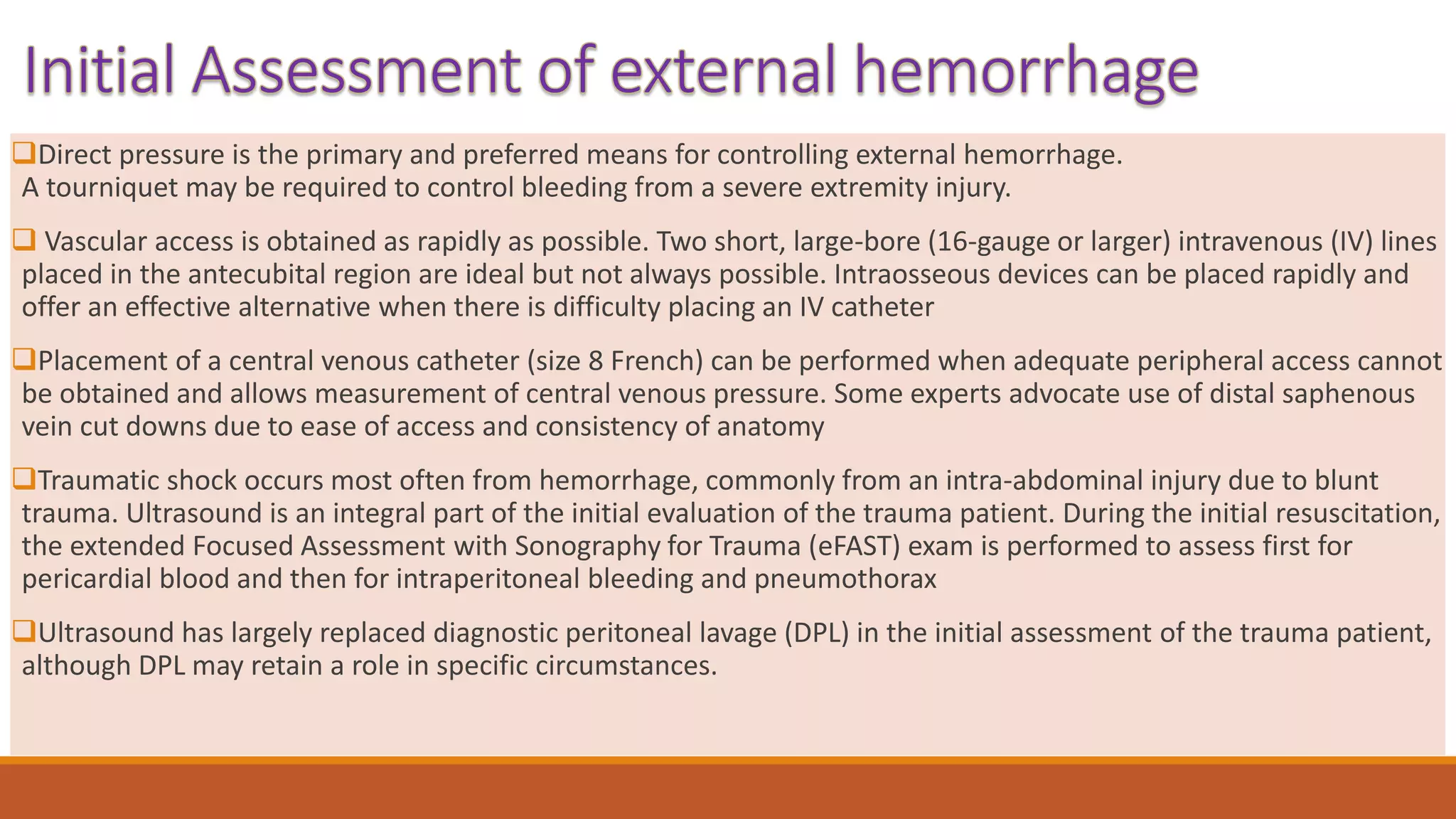
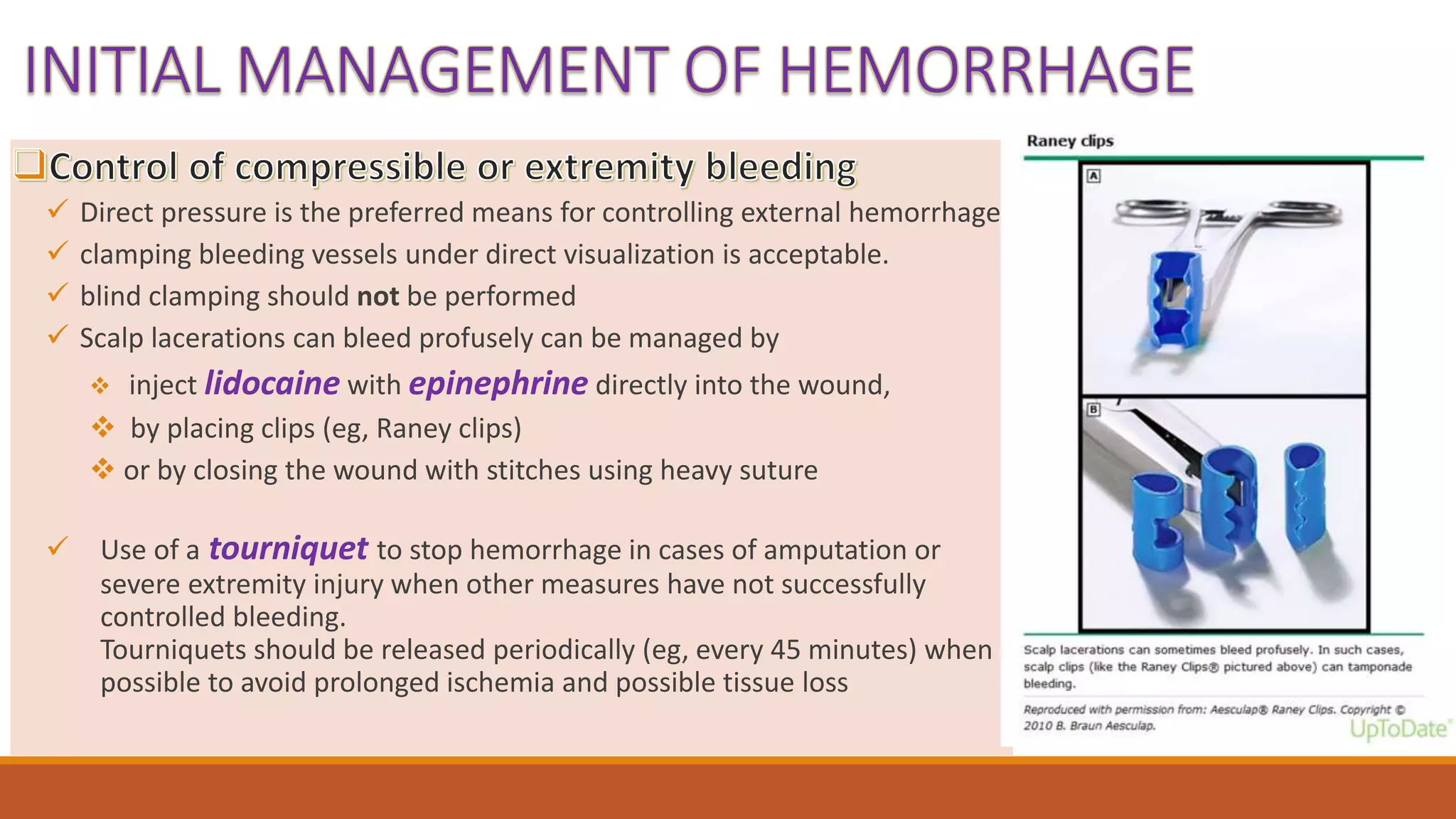
3. Initial assessment of external hemorrhage focuses on recognizing and reversing life-threatening injuries, preventing ongoing blood loss, and restoring intravascular volume. Direct pressure, tourniquets, and hemostatic agents can control bleeding while intravenous fluids, blood products, and rapid mobilization of resources aim to resuscitate the patient.



![ Unstable pelvic fractures and associated vascular injuries
can cause hemorrhagic shock.
Stabilization of the pelvis by applying a circumferential
pelvic
binder or tying a sheet firmly around the pelvis can reduce
bleeding.
Such interventions are most important with "open-book"
pelvic fractures (in which the symphysis pubis is disrupted
[≥2.5 cm], the pelvis opened, and the retroperitoneal
space enlarged)
In addition to immediate orthopedic consultation,
interventional radiology and vascular surgery may be
needed to help control hemorrhage.
This anterior-posterior (AP) radiograph of the pelvis
reveals significant diastasis at the symphysis pubis of
this trauma patient. Such fractures can cause
significant hemorrhage. Emergent treatment consists
of closing the fracture and stabilizing the pelvis by
applying a pelvic binder or tying a sheet tightly around
the lower pelvis.](https://image.slidesharecdn.com/externalhemorrhage-group2-210623223519/75/External-hemorrhage-8-2048.jpg)
![1 2
Controlcompressible andextremity bleeding Minimizetheuse ofintravenous (IV)fluids in
theresuscitation of traumapatients
Give IV fluids only for the resuscitation of
hypotensive patients (eg, MAP <65), and
then only until blood is available
4 5 6
Transfuse bloodproducts assoonas the
need is recognized.
Blood products(ie, red bloodcells, plasma
[clottingfactors],andplatelets) should be
giveninequivalent amounts
Usethromboelastography,or comparable
rapid point-of-careassessment of
coagulation,
to guidetraumaresuscitation whenever
possible.
2
Rapidlymobilizeallneeded resources
(eg, surgery, anesthesia, bloodbank, transfer to
trauma center).
3
in a 1:1:1 ratio. Whole blood can
be used if available](https://image.slidesharecdn.com/externalhemorrhage-group2-210623223519/75/External-hemorrhage-10-2048.jpg)








































































