Downloaded 34 times
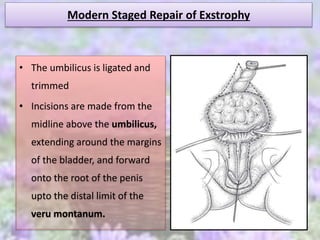
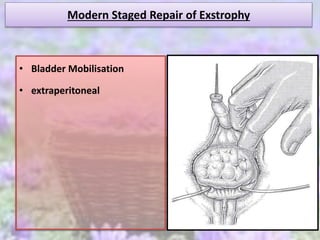
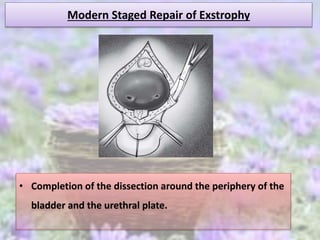
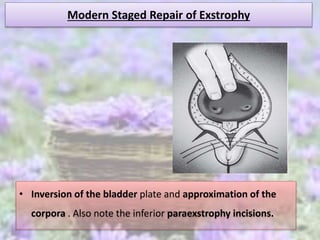
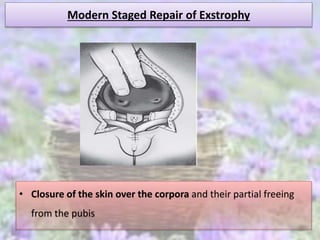
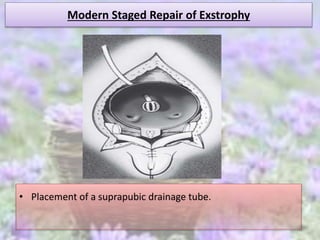
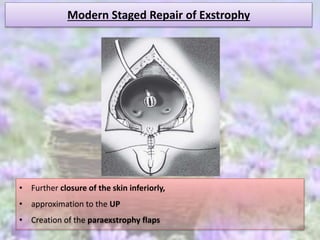
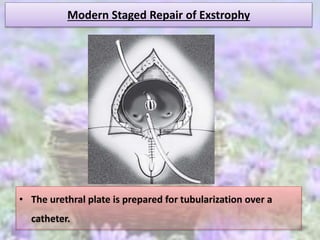
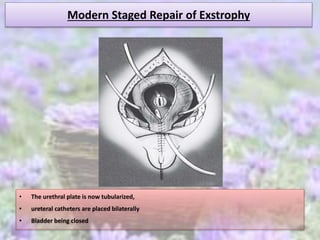
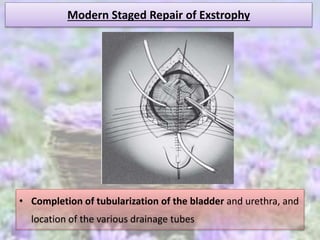
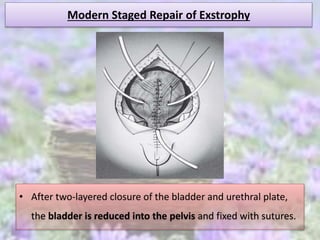
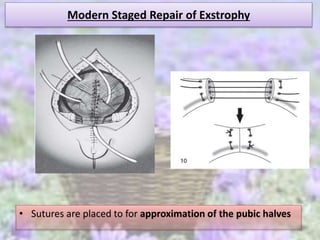
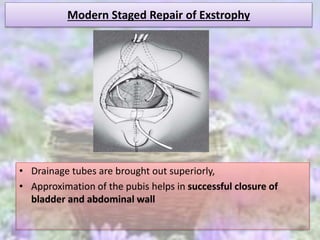
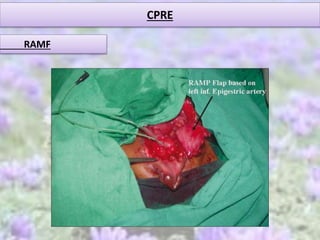
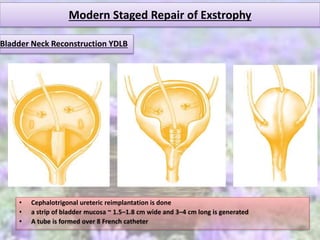
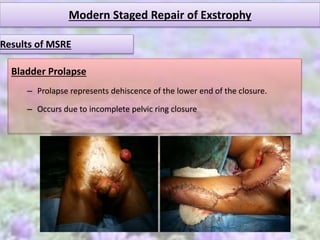

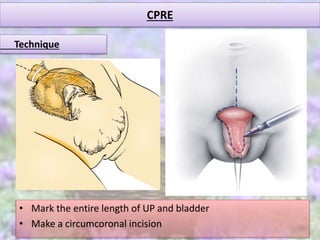
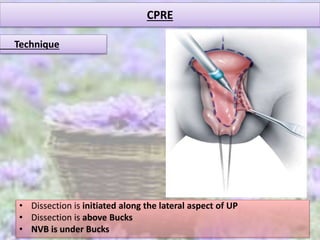
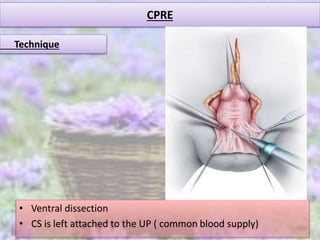
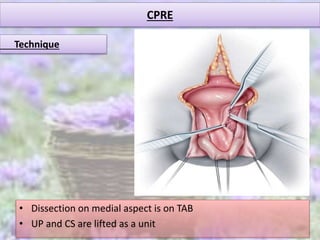
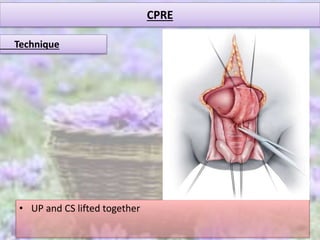
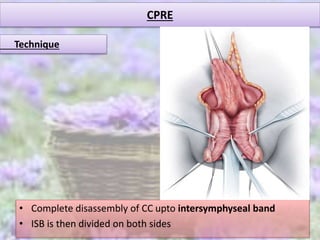
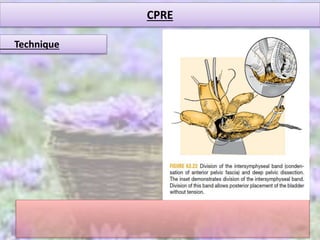
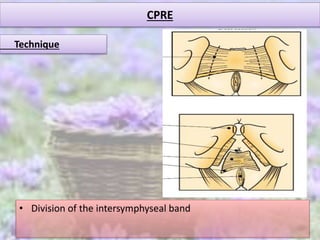
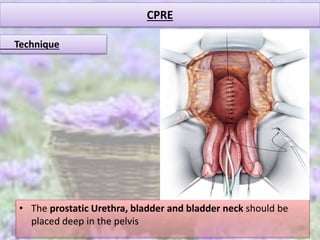
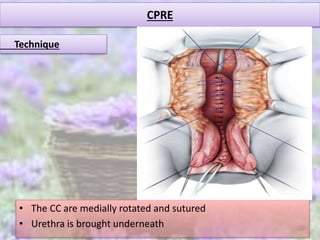
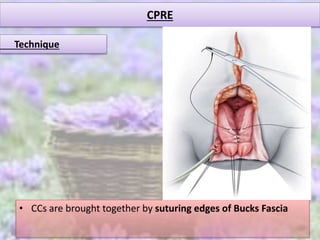


This document discusses modern techniques for repairing exstrophy of the bladder, including: 1. Modern staged repair of exstrophy (MSRE) involves closure of the bladder and urethra at birth, epispadias repair at 6-12 months, and bladder neck reconstruction at 4-5 years when bladder capacity is adequate. 2. Complete primary repair of exstrophy (CPRE) simultaneously closes the bladder, abdominal wall, and repairs epispadias to decrease costs and morbidity from multiple surgeries. 3. Techniques are described for MSRE bladder closure, epispadias repair using the Cantwell-Ransley technique, and CPRE involving complete dis






















































































