
Recommended
More Related Content
What's hot
What's hot (20)
Similar to abdallahamad04@gmail.com
Similar to abdallahamad04@gmail.com (20)
Recently uploaded
Recently uploaded (20)
abdallahamad04@gmail.com
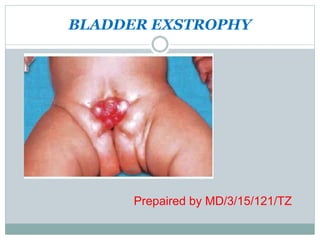
- 1. BLADDER EXSTROPHY Prepaired by MD/3/15/121/TZ
- 2. CONTENTS 1. Introduction 2. Epidemiology 3. Etiology- Risk Factors 4. Pathology 5. Clinical features- Symptoms & Signs 6. Differential diagnosis 7. Investigations 8. Treatment
- 3. ANATOMY OF URINARY BLADDER It is a muscular reservoir of urine situated in the pelvis, posterior to the pubic bone separated by the retro-pubic space. The size, shape, position of bladder vary depends on amount of urine it contains Made up of detrusor and trigone muscles The neck of bladder is of 3-4 cm
- 5. BLOOD SUPPLY Superior vesical artery, a branch of internal iliac artery. Inferior vesical artery. – Venous drainage is by the vesical plexus of veins, which drains into the internal iliac veins.
- 6. INNERVATION AND LYMPHATIC DRAINAGE Lymphatics drain into internal iliac and external iliac nodes. The efferent parasympathetic fibres (S2-S4): contraction of the detrusor muscle and relaxation of the sphincter vesicae. The sympathetic input, this arises in the 11th thoracic to the second lumbar segments;
- 7. By definition:is defined as incomplete development of the infraumbilical part of the anterior abdominal wall and anterior wall of the bladder . This is one among the commonest congenital abnormality lower urinary and genital track
- 8. EPIDERMIOLOGY Occurring approximately 1/3000 of all child birth Males are more often affected than females by the ratio is 5 : 1 to 6:1
- 9. RISK FACTORS It occurs in infants of young mother Inrease 10 folds to those mothers who received high dose of progestrone during the first trimester
- 10. PATHOPHYSIOLOGY Abnormal large cloacal membrane prevents the mesodermal to growth and lower abdominal midline fusion. So when the cloacal membrane rupture the anterior abdominal wall,pubis,bladder and urethra fail to develop normally
- 11. TYPES There are two types 1.complete 2. incomlete: the pubic bones are united and the external genitalia normal or there is epispadias.
- 12. CLINICAL PRESENTATION Anterior abdominal wall absent Posterior bladder linning which is bright red color is exposed Urine seeps into the posterior bladder wall from abnormal ureteral outlets At time of birth the mucosa of bladder may be thin and smooth but it is later become edemetous
- 13. ASSOCIATED ANOMALIES: 1. The rami of pubic bones are widely separated. There is a thick fibrous band. The femurs are rotated externally and the child waddles like a duck (waddling gait). 2. The umbilicus is absent. There may be umbilical hemia.
- 14. 3. Genitalia.— (a) In the males : (i) Epispadias is almost always present. (ii) The penis is broader and shorter than normal. It is drawn up and fixed to the abdominal wall. (iii) The scrotum may be ill-developed. (iv) The testes may be normal or ectopic or maldescended. (v) The prostate and seminal vesicles are often rudimentary or absent.
- 15. (b) In the females : (i) The clitoris is usually cleft. (ii) The labia minora are separated. (iii) There may be anomalies in the development of uterus and vagina. 4. Anal sphincter is often lax. 5. Hernia : (a) Umbilical hernia may be present. (b) There may be inguinal hernia of one or both sides
- 16. COMPLICTIONS Hemorrhage Ulceration Pain Recurrent pyelonephritis Renal failure Metaplastic changes in mucosa can lead into adenocarcinoma 50% of patients die of renal failure
- 17. DIAGNOSIS 1 Diagnosis: can be confirmed before delivery via uss and or MRI. Also clinically 2 Diffential diagnosis: patent urachus
- 18. INVESSTIGATION prenatal USS: include a lower abdominal wall mass, absent bladder filling, low-set umbilicus, small genitalia, abnormal iliac crest widening. Diagnosis can help planning of delivery in a centre with facilities to perform early surgical correction.
- 19. MANEGEMENT At birth: cover the bladder with plastic fi lm and irrigate regularly with sterile saline. Surgical: Newborn: pelvic osteotomy (cutting bone to correct deformity) with external fixation and closure of bladder, abdominal wall, and posterior urethra.
- 20. 6–18 months: epispadias repair 4–5yrs: bladder neck reconstruction (Young– Dees– Leadbetter procedure) and anti-reflux surgery (ureteric re-implantation)is performed when there is adequate bladder capacity and children can participate in voiding protocols. Where bladder capacity is too small, bladder augmentation and/or urinary diversion is required
- 21. SURGICAL COMPLICATION :increased risk of malignancy in urinary or orthotopic bladder fistula hypospadias bladder stones infection (UTI, epididymitis) incontinence
- 22. AHSANTENI THANKS VERY MUCH FOR ALL THANKS AHSANTENI