Downloaded 21 times



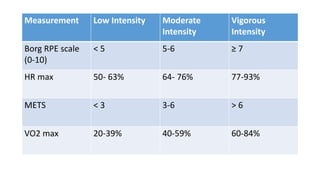
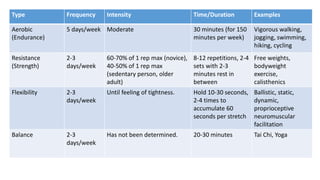

Exercise prescription is a structured activity plan designed to improve patient health, addressing various conditions like asthma, diabetes, and obesity. It emphasizes the FITT principles (Frequency, Intensity, Type, Time) and involves pre-exercise screenings to assess cardiovascular risks, along with tailored exercise programs, especially for cancer and cardiac patients. The document details aerobic and resistance training guidelines, the importance of progression, and the physiological benefits of regular physical activity.



































































