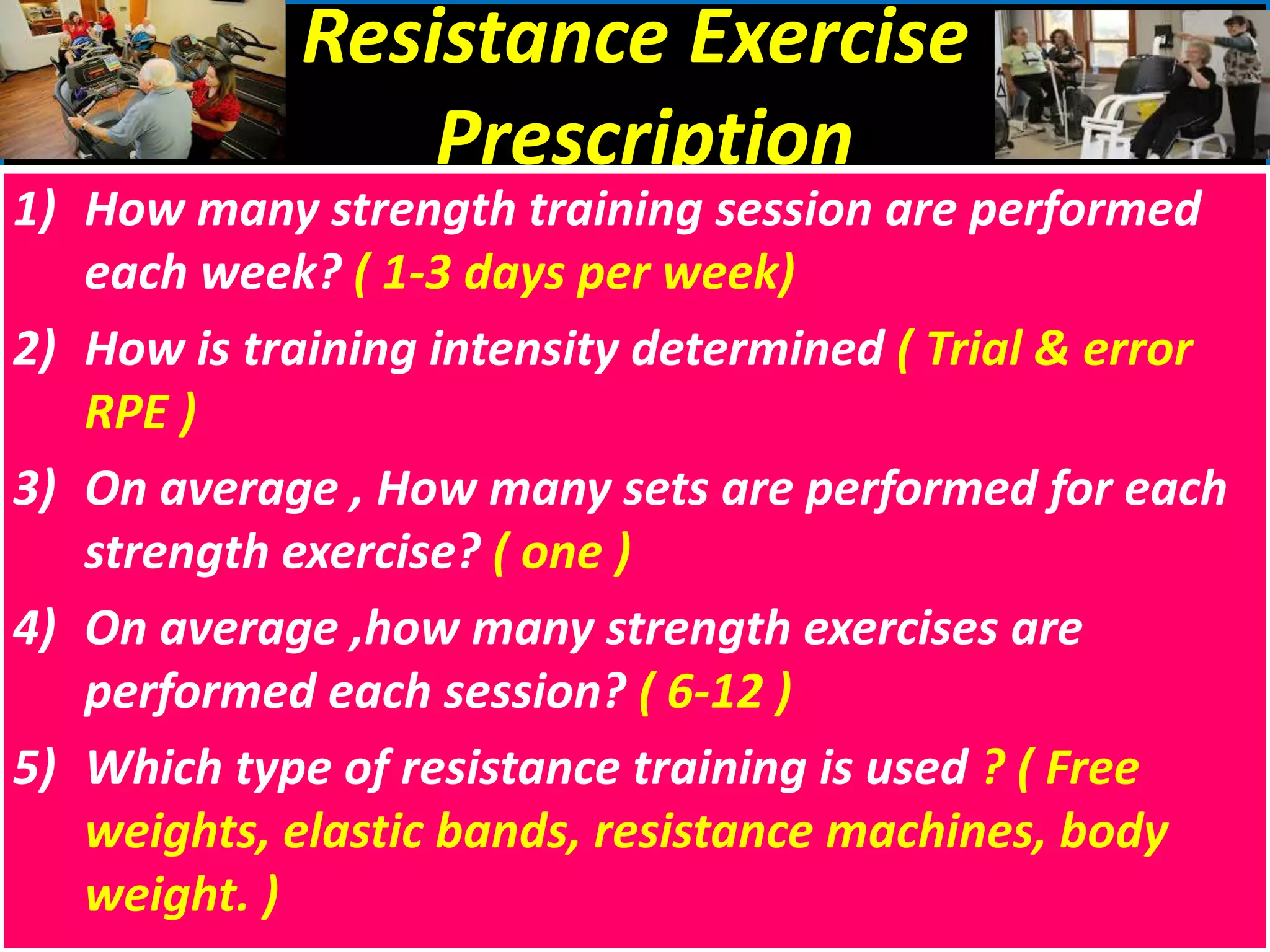
This document provides information on exercise prescription for cardiac rehabilitation. It discusses assessing patient risk and stratifying them before creating an individualized exercise plan. The goals of a cardiac rehabilitation program are to improve exercise capacity and reduce cardiac ischemia through aerobic and resistance training 3 times per week for 30 minutes each session at a target heart rate of 70-85% of maximum. Contraindications include unstable angina or new symptoms during exercise. Baseline testing establishes work capacity and excludes issues before developing a safe prescription.

























































![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)



























































