Downloaded 58 times





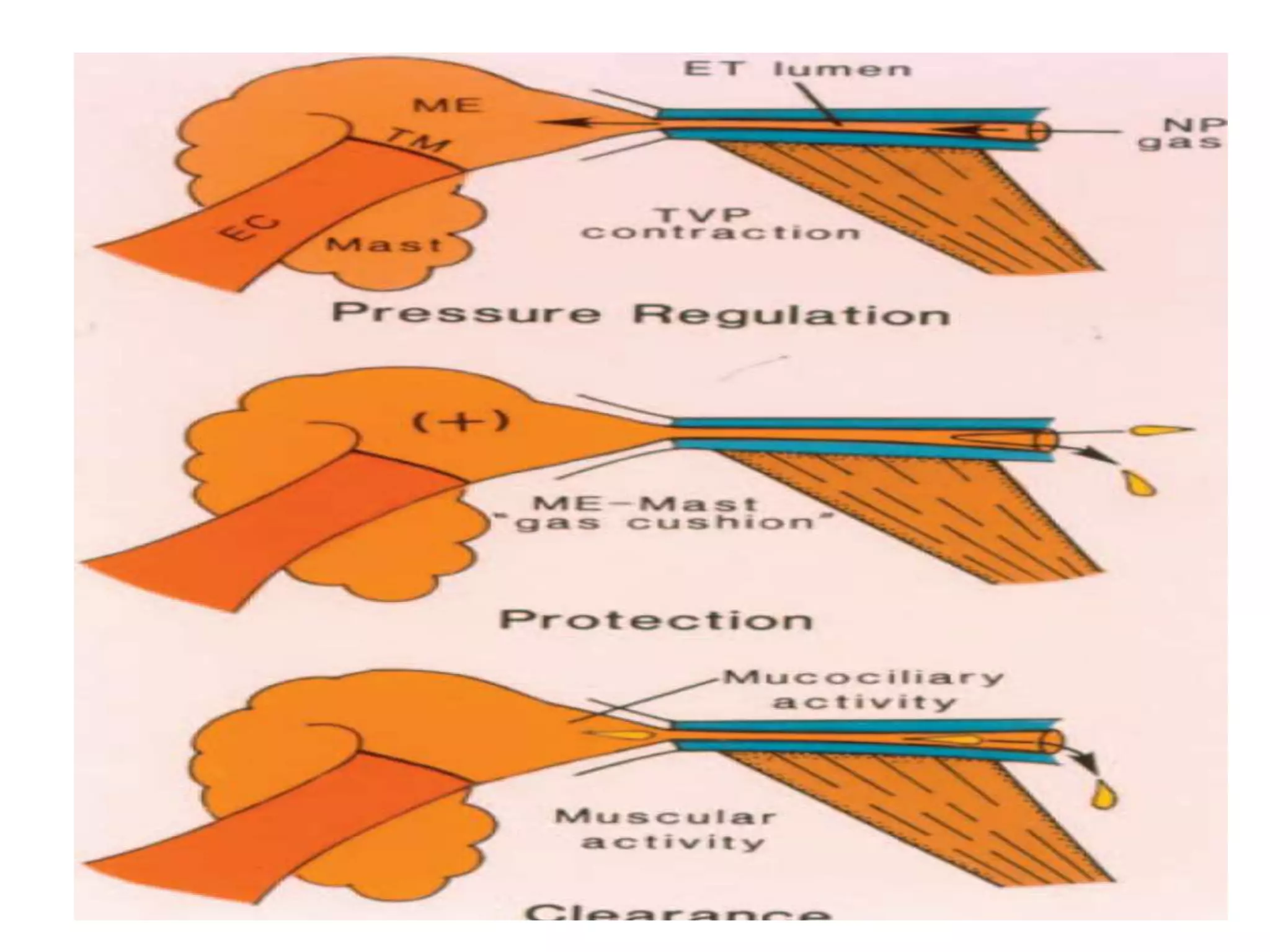









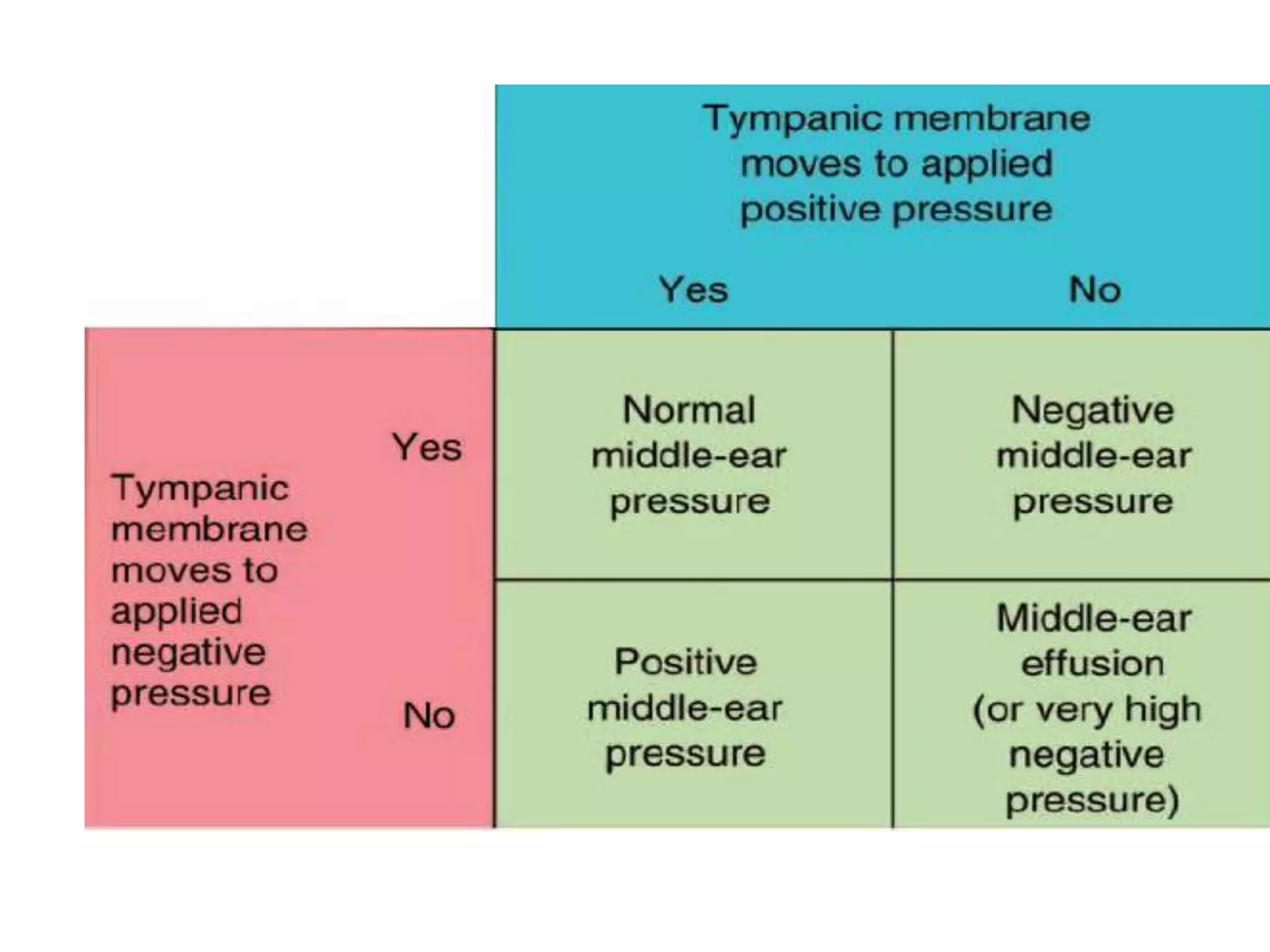

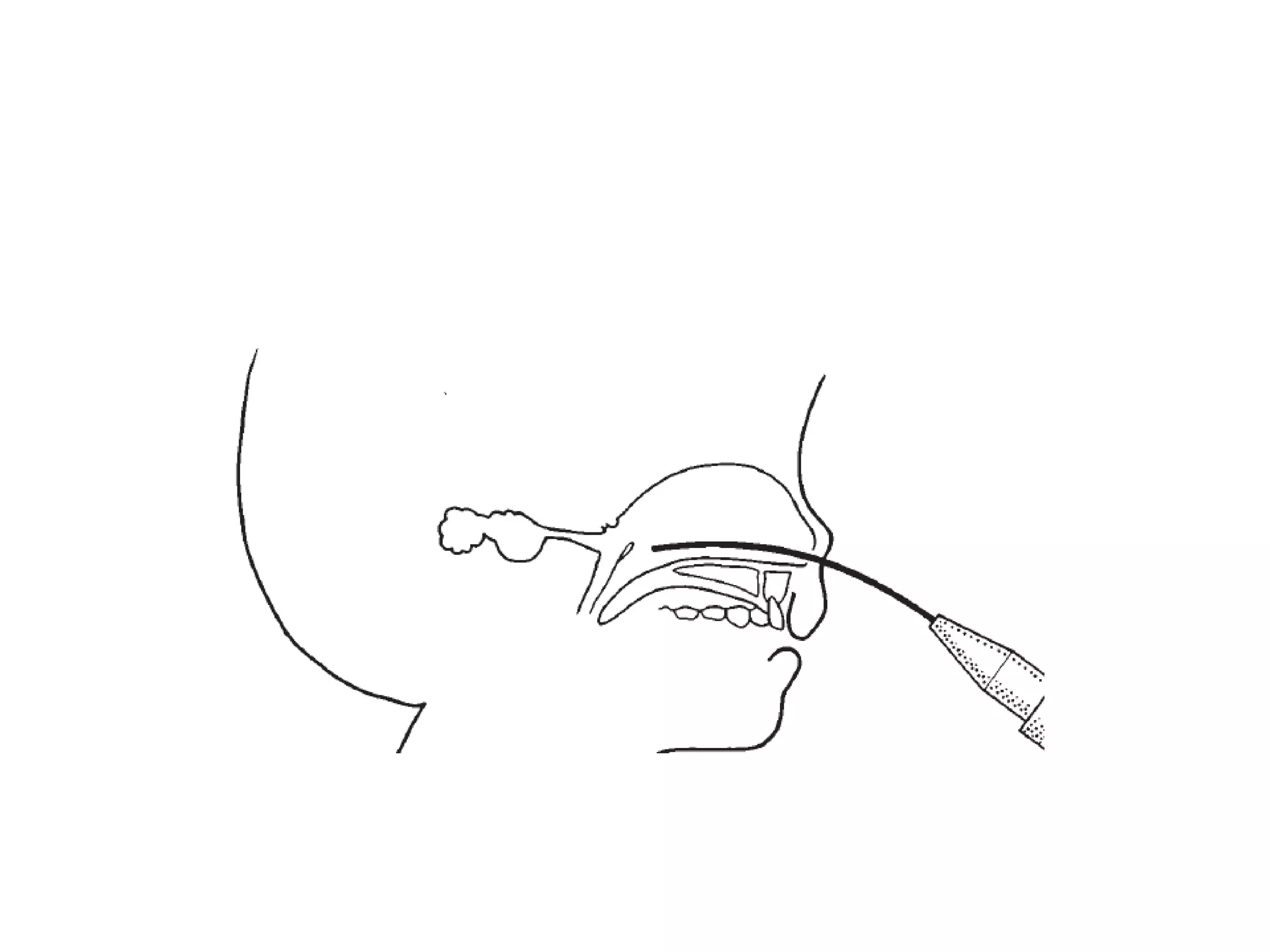




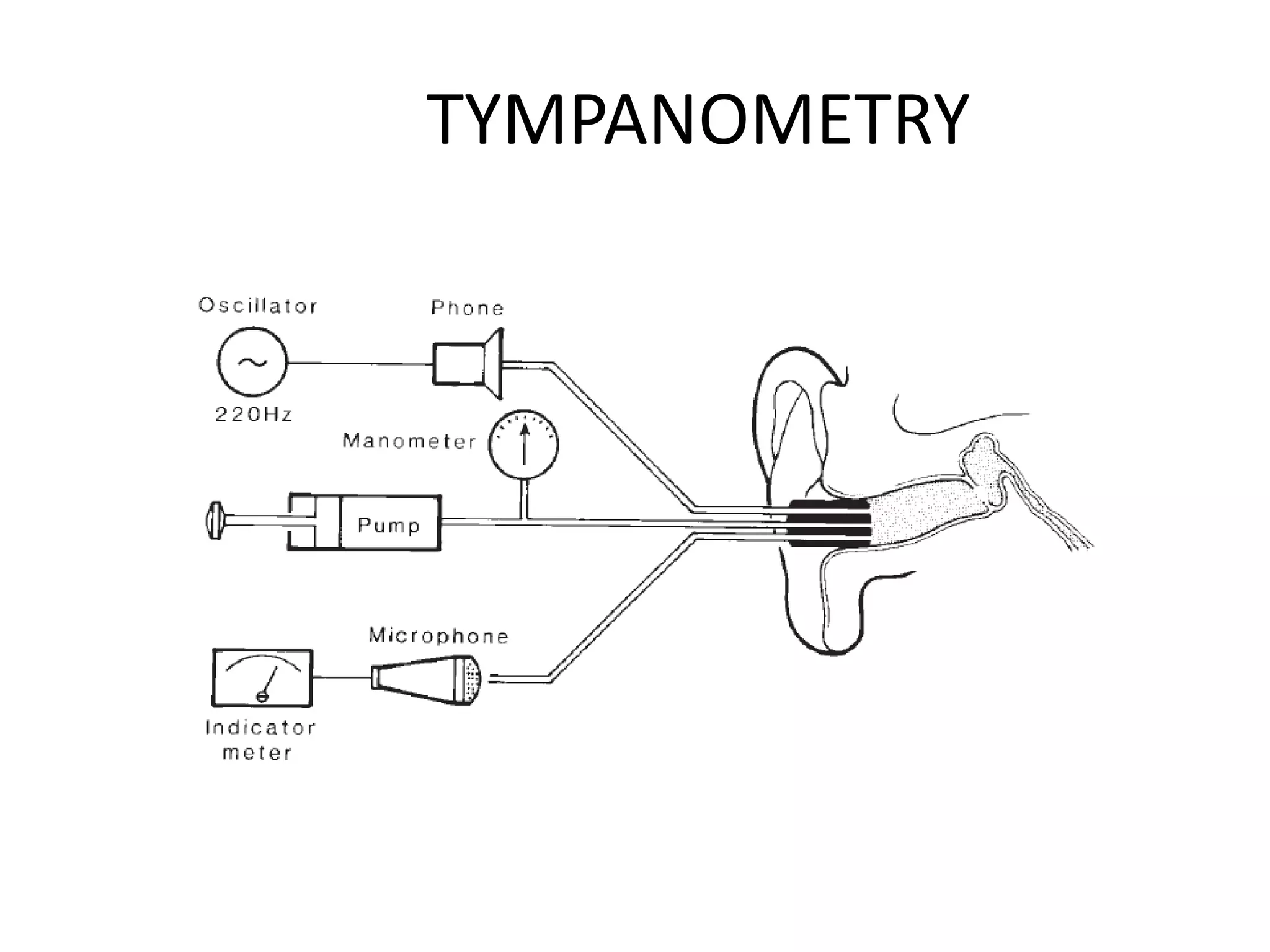








The eustachian tube functions to equalize pressure between the middle ear and external environment, clear mucus from the middle ear, and protect the middle ear. It develops from the first pharyngeal pouch during embryology. Assessment of eustachian tube function involves history, physical exam including pneumatic otoscopy, and tests like Valsalva maneuver, Politzer's test, and tympanometry. Dysfunction can be caused by problems with mucociliary clearance, surfactant, or patulousness of the tube. Evaluation of patency uses techniques like nine-step testing, sonotubometry, and manometry.




















































































