Downloaded 61 times




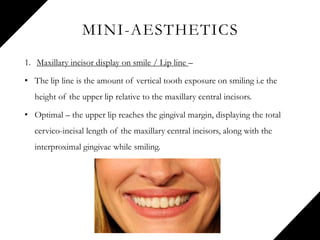
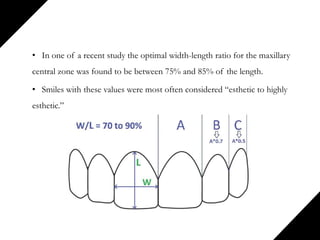
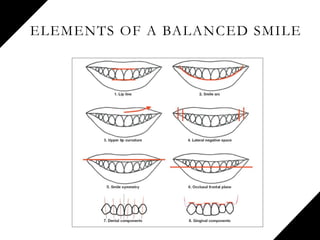
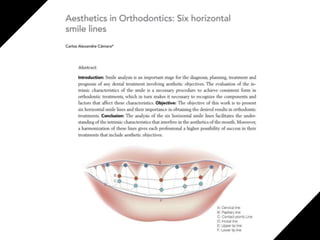
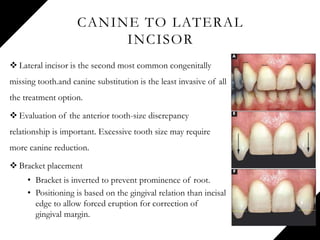
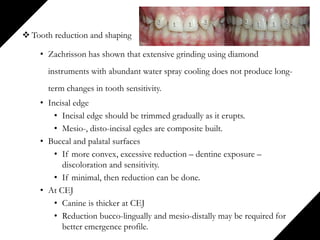


The document presents a comprehensive overview of esthetics in orthodontics, covering topics such as the historical context, psychological and functional assessments for smile design, and specific aesthetic principles like macro, mini, and micro-aesthetics. It emphasizes the importance of understanding individual patient perceptions and desires while balancing health, function, and aesthetic goals in orthodontic treatment, particularly for issues like deep overbite and gummy smiles. The document also details the methodologies and treatment strategies necessary for achieving aesthetically pleasing smiles.







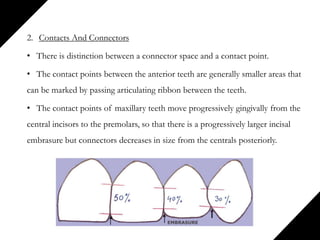
![Loops in orthodontics and its uses [Autosaved]..ppt](https://cdn.slidesharecdn.com/ss_thumbnails/loopsinorthodonticsautosaved-241204161830-0e1eccec-thumbnail.jpg?width=640&height=640&fit=bounds)








































































