Downloaded 23 times
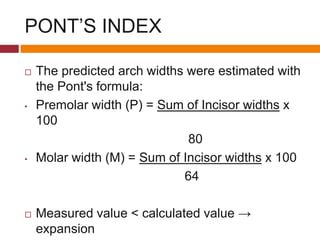
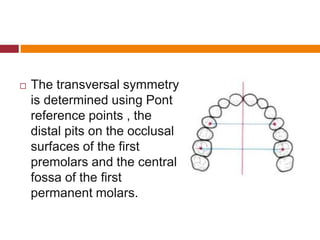
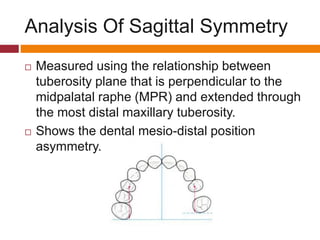
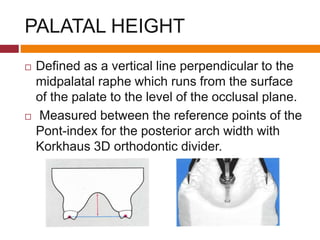
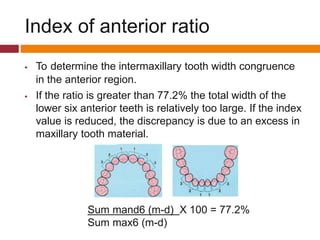


The document discusses essential and supplemental diagnostic aids used in orthodontics, providing a comprehensive overview of various analyses, including dental arch width, pont’s index, and space analysis. Key methods for assessing malocclusions and treatment planning are outlined, emphasizing the importance of a thorough diagnosis that incorporates clinical aids, radiographs, and cast analysis. It also highlights various parameters related to the dental arches, including symmetry, palatal height, and tooth size discrepancies, crucial for effective orthodontic practice.


































































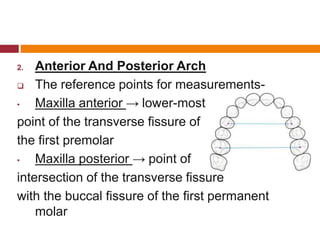
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









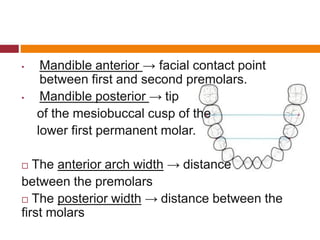
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




