Downloaded 30 times














![12 y/o M for VATS biopsy
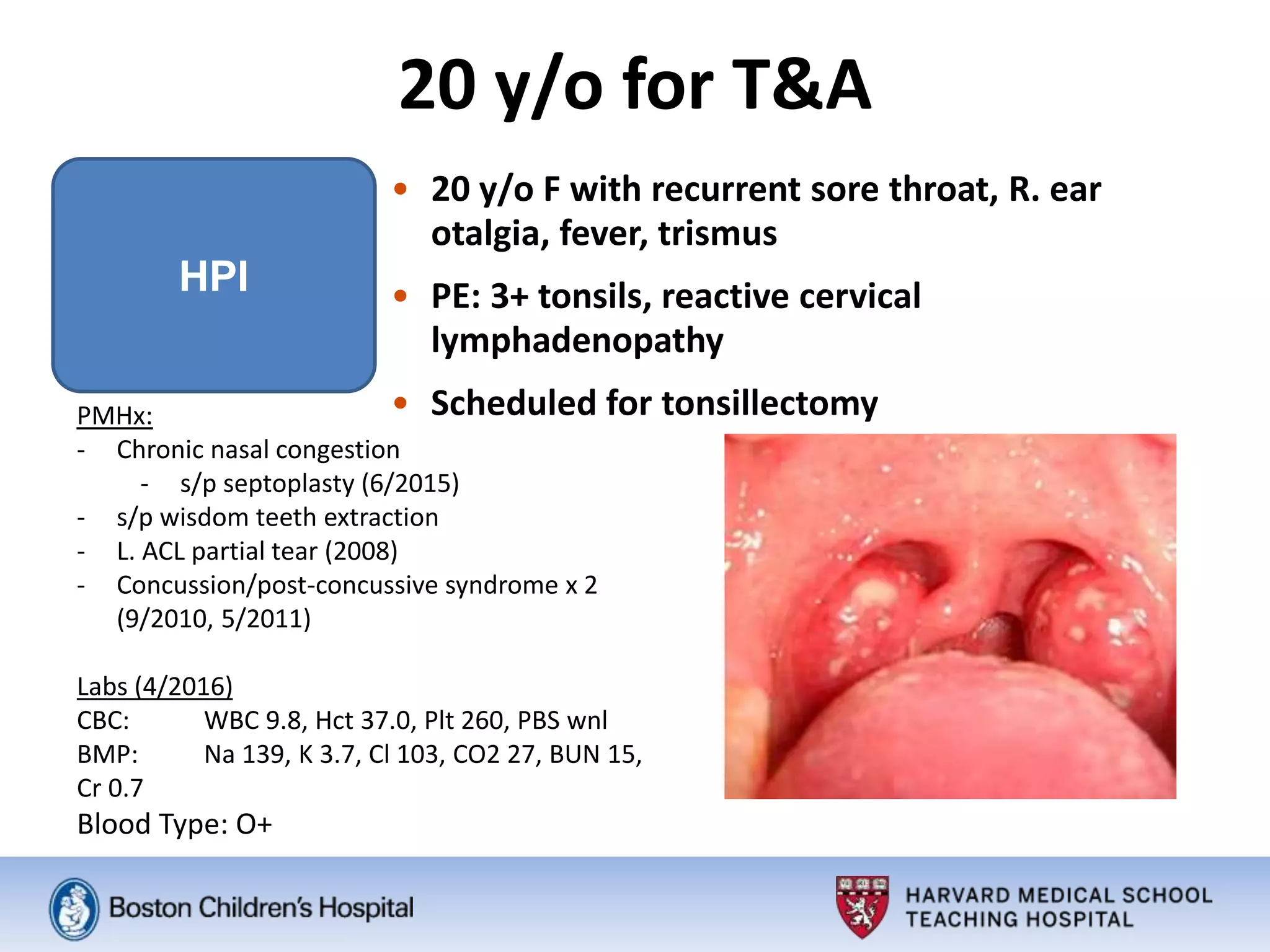
HPI
• P/w fever, cough, myalgias, congestion, nausea,
vomiting, sore throat, intermittent H/A
• Dx PNA 3 months ago with mild R. pleural effusion
• Treated with CTX complete resolution (per CXR)
PMHx: Born at at 31wks, 2-wks in NICU intubated; Otherwise Healthy
SocHx: From Sudan, travelling through Istanbul to US
PE: Lethargic
- CBC: [6/2]: WBC 5.5, Hct 36, PLT 455; ESR 62, CRP 10, LDH 176 264
- CXR [6/2]: RML/RLL consolidation + R. effusion: c/fPNA + parapneumonic effusion
- CT [6/2]: R. pleural effusion with pleural thickening,
mediastinal + hilar LN: c/f empyema
- Nl ECHO, respiratory cultures, ANA, pleural fluid flow cytometry and various bacterial/fungal cx
Received CG in Sudan, started on Vancomycin/ceftriaxone at BCH
- To IR 6/3: PICC, 10Fr pigtail CT 825 ml serous straw-colored fluid (+400cc up to 6/10)
- Negative induced sputum AFB x 3, but persistent fevers…
- 6/8: Positive Tspot and slightly elevated ADA (suggestive of isolated TB effusion) VATS](https://image.slidesharecdn.com/1264dab2-f3f3-40cf-b875-04c2e24aa61e-160710034633/75/Post-Tonsillectomy-Bleed-and-One-Lung-Ventilation-Anesthetic-Management-17-2048.jpg)








![Thank You!
• Jue Wang, MD
• Thomas Mancuso, MD [Course Director]
• Carlos Munoz-San Julian, MD; Izabela Leahy,
RN BSN MS [Course Planners]](https://image.slidesharecdn.com/1264dab2-f3f3-40cf-b875-04c2e24aa61e-160710034633/75/Post-Tonsillectomy-Bleed-and-One-Lung-Ventilation-Anesthetic-Management-26-2048.jpg)

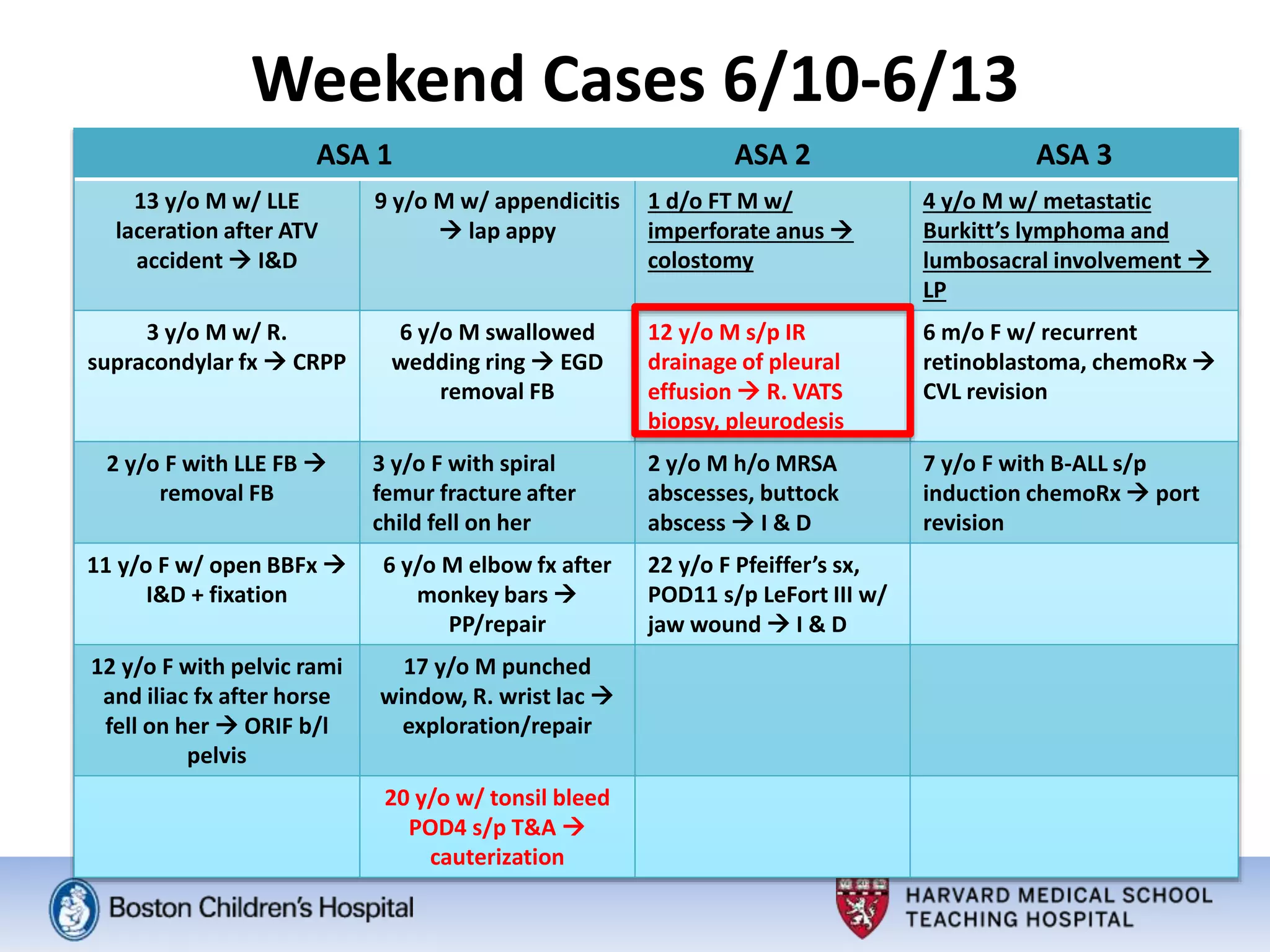
The morning report summarizes 18 surgical cases from June 10-13. The majority of cases were ASA class I or II. The largest proportion of cases were from general surgery. A post-tonsillectomy bleeding case on postoperative day 5 required cauterization. Key considerations for one-lung ventilation were discussed for a 12-year-old undergoing VATS biopsy for possible tuberculosis including goals for oxygen saturation and approaches for addressing hypoxemia.










































































