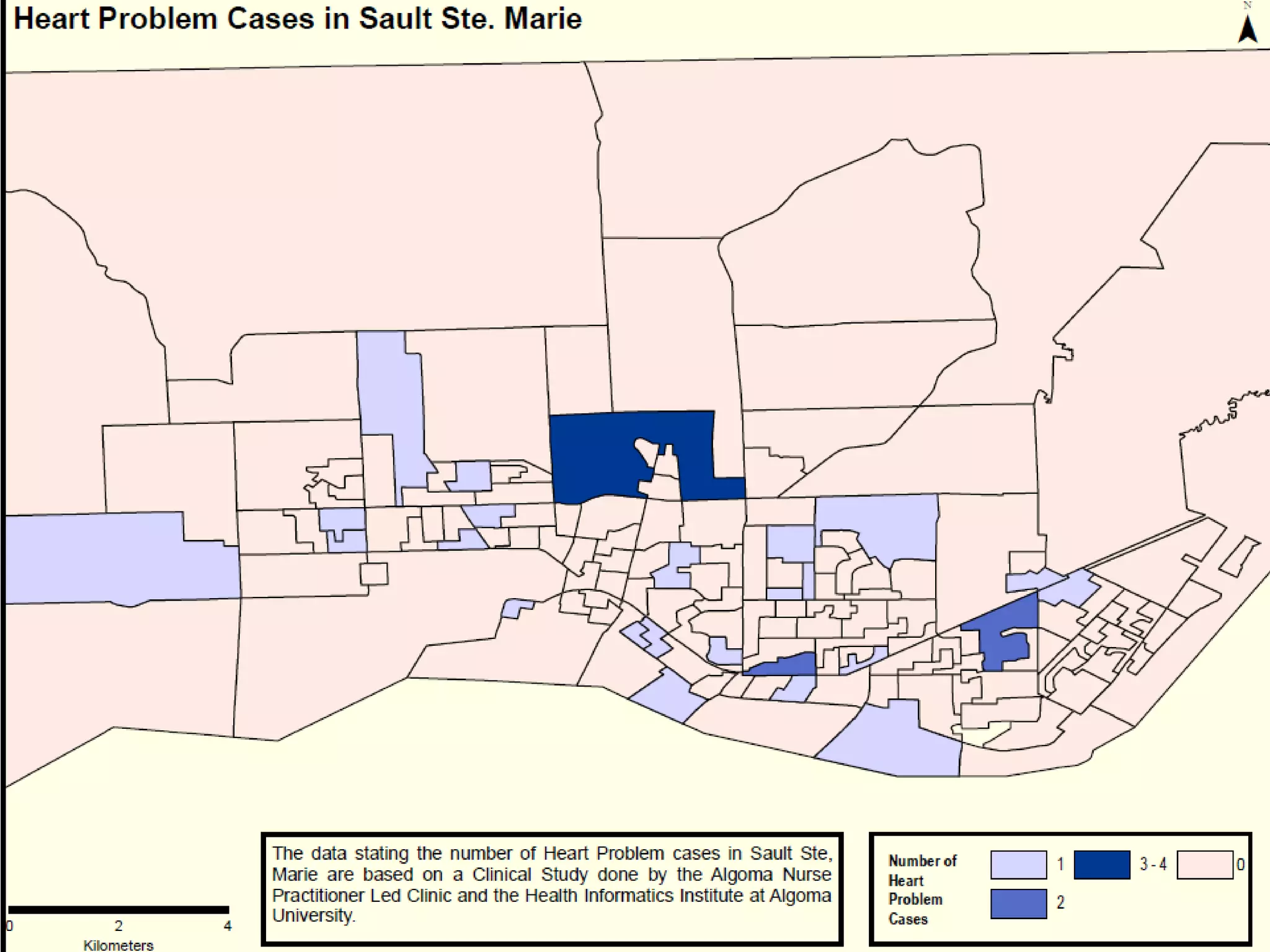
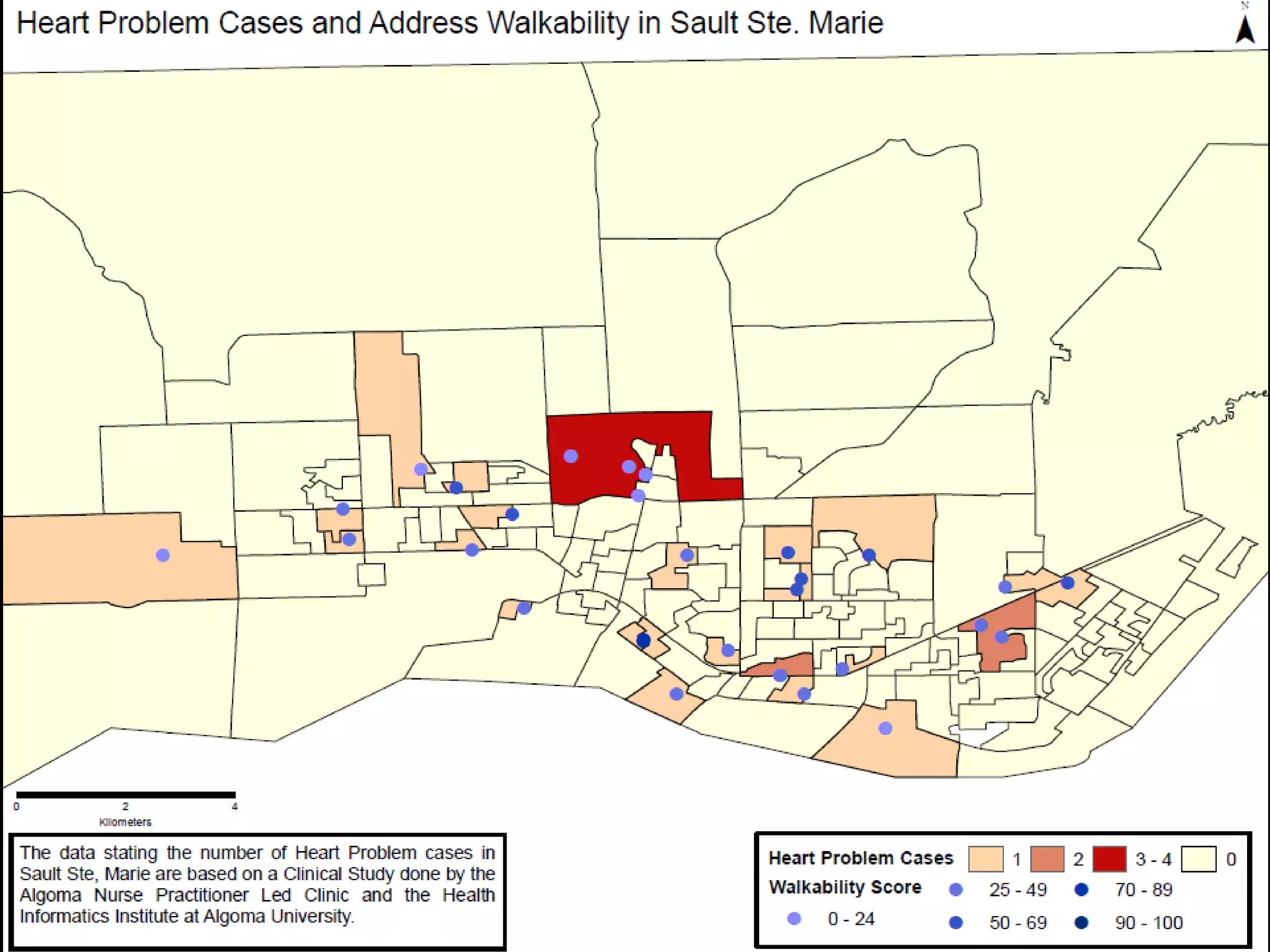
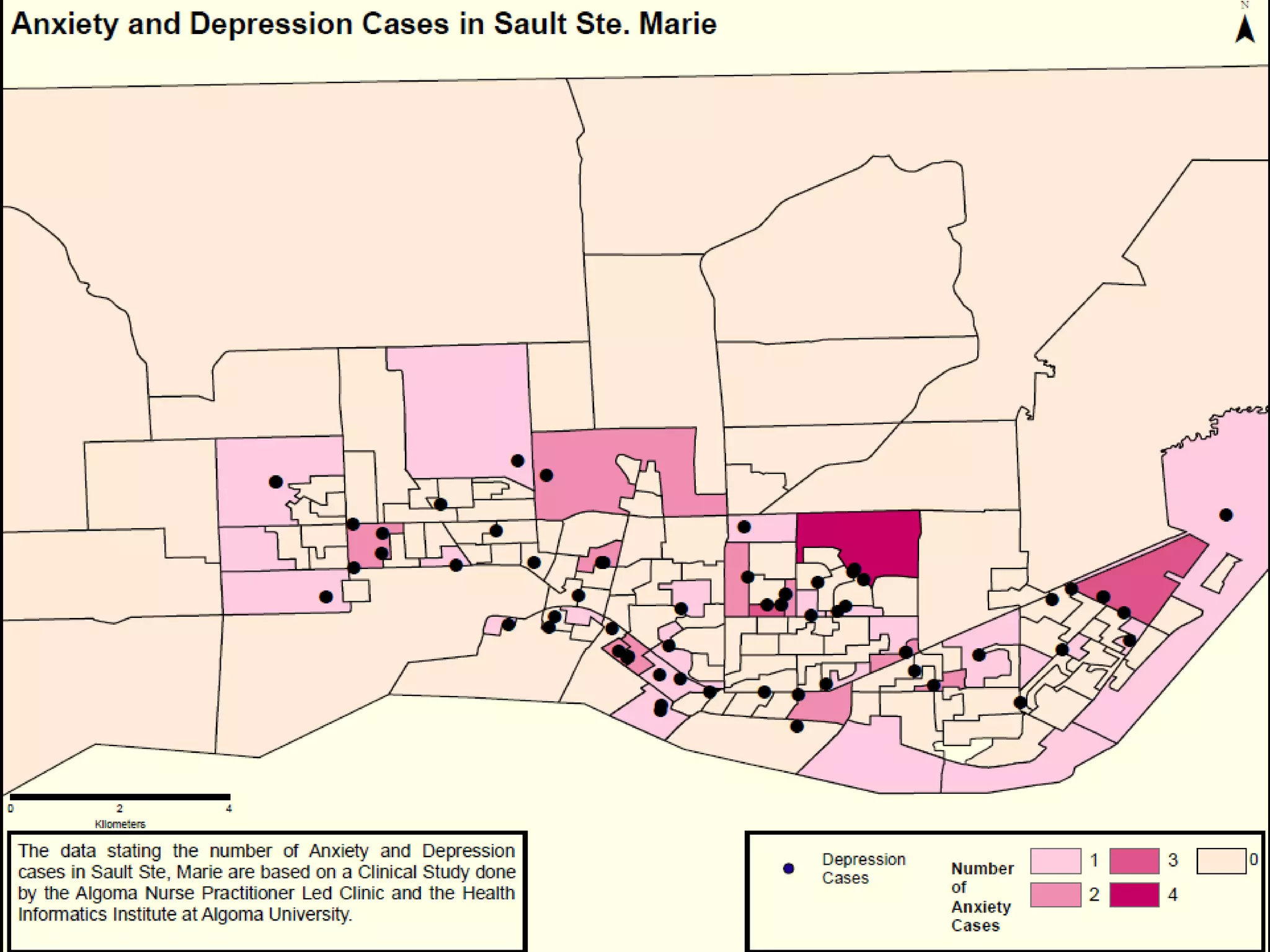
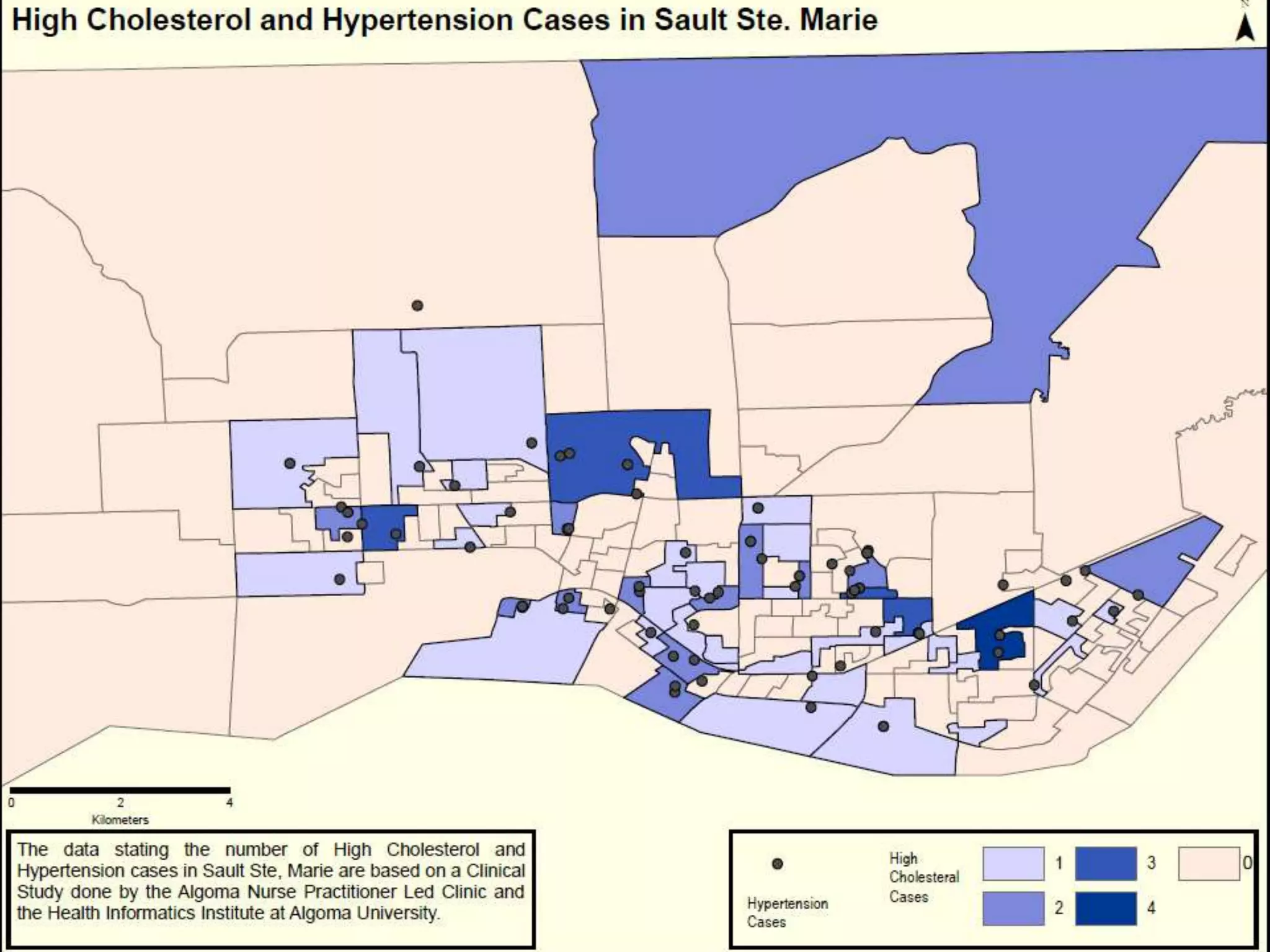
This document summarizes a GIS analysis study conducted by the Health Informatics Institute – Algoma University to understand chronic disease risk factors in the Algoma Region and facilitate individualized care plans. Over 1,000 patients were recruited through mailed surveys and phone calls. Geographic, health, and socioeconomic data were collected and layered in a GIS analysis. This identified relationships between behavioral, environmental, and demographic attributes and health issues. The results provided insights into the patient population to guide more personalized care. Future studies could replicate successful recruitment methods and apply findings to both individual patient care and public health promotion.






































![Structured Forests for Fast Edge Detection [Paper Presentation]](https://cdn.slidesharecdn.com/ss_thumbnails/mc-crpresentation-141209192730-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Urban transportation policy program]city paper presentation guangzhou](https://cdn.slidesharecdn.com/ss_thumbnails/urbantransportationpolicyprogramcitypaperpresentationguangzhou-160407030338-thumbnail.jpg?width=640&height=640&fit=bounds)