This document discusses epistaxis (nosebleeds), including:
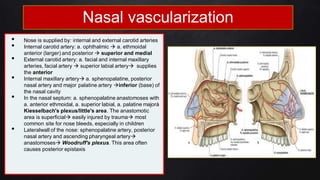
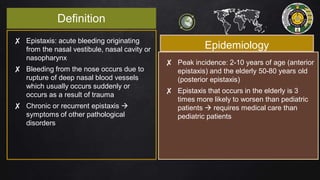
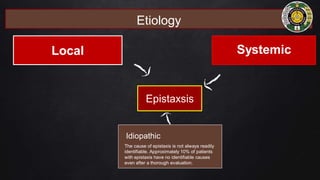
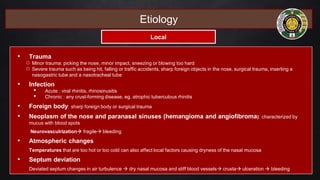
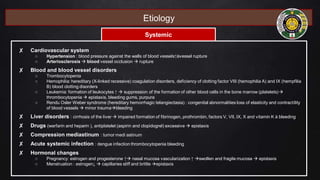
1. Epistaxis is a common ENT emergency caused by rupture of blood vessels in the nose from trauma, infections, or systemic diseases. It can be mild and self-limiting or severe and life-threatening.
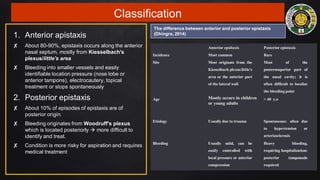
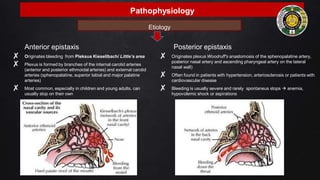
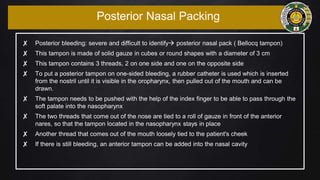
2. Epistaxis is classified as anterior (originating in front of the nose) or posterior (originating further back). Anterior epistaxis is more common and usually milder.
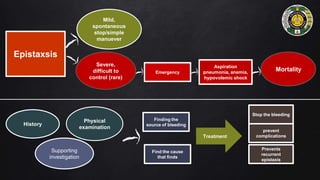
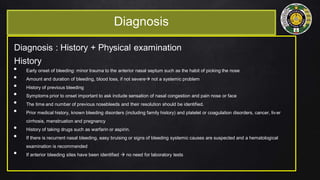
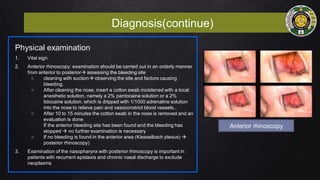
3. Diagnosis involves history, physical exam including anterior rhinoscopy, and potentially laboratory tests or imaging if the source of bleeding cannot be found or if a systemic condition is suspected.
![References
• American Rhinologic Society. 2015. Epistaxis (Nosebleeds). ARS [Internet]. Available from:
http://care.americanrhinologic.org/epistaxis
• David, A. R, M., 2020. ‘Simplified management of epistaxis’. Journal of the American Association of Nurse Practitioners,
00(00), pp. 1-5
• Dhingra, P. L., Dhingra, S. 2014. Epistaxis in Diseases of Ear, Nose and Throat Head & and Neck Surgery, 4th edn.
Elsevier. India, pp: 4-5, 70., 4th edn, Elsevier, India, pp. 176-180
• Guyton and Hall, 2016, Textbook of Medical Physiology, Canada : Elsevier
• Jason, P. W. M., Jill, K. M., Marissa, J. S. D. 2018. ‘Epistaxis: Outpatient Management’. Rutgers University Robert Wood
Johnson Medical School, New Brunswick, New Jersey, vol. 98(98), pp. 240
• Lee, S. M., Kim, Y. M., & Kim, B. M. 2016. Epistaxis as the First Manifestation of Silent Renal Cell Carcinoma: A Case
Report with Relevant Literature Review. Iranian journal of radiology : a quarterly journal published by the Iranian
Radiological
• Mangunkusumo, E., Retno, S. W. 2007, Epistaksis. Perdarahan Hidung dan Gangguan Penghidu in Ajar Ilmu Kesehatan
Telinga Hidung Tenggorok Kepala & Leher, 6th edn, ed. Soepardi, E. A, FK UI, Jakarta, pp. 155-159
• Netter, F. H., 2016, Atlas Anatomi Manusia, Singapore : Elsevier
• Nguyen, Q. A. 2020. ‘Epistaxis’. Drugs and Diseases: Otolaryngology and Facial Plastic Surgery. Medscape. Department
of Otolaryngology-Head and Neck Surgery, University of California, Irvine, Medical Center. Available from:
https://emedicine.medscape.com/article/863220-overview#a6
• Paulsen, F., Waschke, J., 2012. Sobotta : Atlas Anatomi Manusia, 23rd ed. Penerbit Buku Kedokteran (EGC), Jakarta](https://image.slidesharecdn.com/slidereferatepistaxisimanueldarbiantorosihotang1-220219160505/85/Epistaxis-34-320.jpg)
![References
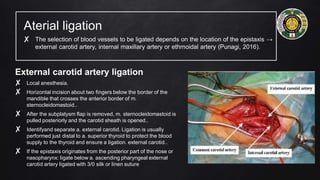
• Punagi, A. Q. 2016. Epistaksis. Sistem Trauma dan Kegawatdaruratan. Fakultas Kedokteran Universitas Hasanuddin.
Makassar, pp. 1-30
• Purnama, H. 2014. Penatalaksanaan Epistaksis. RSUD. Kabupaten Bekasi, pp. 1-7
• Qureishi, A., Burton, M. J. 2012. Interventions for recurrent idiopathic epistaxis (nosebleeds) in children. Cochrane
Database Syst Rev, vol. 9:CD004461
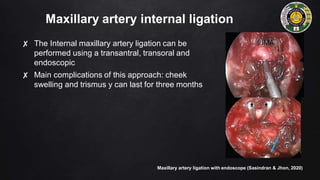
• Sasindran, V., & John, M. S. 2020. Role of Endoscopic Internal Maxillary Artery Ligation in Intractable Idiopathic
Epistaxis. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of
Otolaryngologists of India, 72(2), 228–233. https://doi.org/10.1007/s12070-020-01788-y
• Soetjipto, D., Mangunkusumo, E., Retno, S. W. 2007, Hidung in Ajar Ilmu Kesehatan Telinga Hidung Tenggorok Kepala &
Leher, 6th edn, ed. Soepardi, E. A, FK UI, Jakarta, pp. 119-122
• Swift, A. C., Bleier, B. S., Bhalla, R. K., Schlosser, R. J. 2013. Epistaxis: etiology, investigation and management. In
Rhinology and skull base surgery from lab to the opening room: an evidence based approach. Thieme Medical publisher,
New York,USA, pp. 507-523
• Tabassom, A., Cho, J. J. 2022. ‘Epistaxis’. In: StatPearls [Internet]. Treasure Island (FL). Available from:
https://www.ncbi.nlm.nih.gov/books/NBK435997/
• Tunkel, D. E., Anne, S., Payne, S. C., Ishman, S. L., Rosenfeld, R. M., Abramson, P. J., Alikhaani, J. D., Benoit, M. M.,
Bercovitz, R. S., Brown, M. D., Chernobilsky, B., Feldstein, D. A., Hackell, J. M., Holbrook, E. H., Holdsworth, S. M., Lin, K.
W., Lind, M. M., Poetker, D. M., Riley, C. A., … Monjur, T. M. 2020. Clinical Practice Guideline: Nosebleed
(Epistaxis). Otolaryngology–Head and Neck Surgery, 162(1_suppl), S1–S38. https://doi.org/10.1177/0194599819890327
• Zahra, S.S., 2016, 'Anatomi dan Fisiologi Hidung'. Jurnal Kedokteran UNDIP, vol.7. no. 19, pp.23-30](https://image.slidesharecdn.com/slidereferatepistaxisimanueldarbiantorosihotang1-220219160505/85/Epistaxis-35-320.jpg)




































































