Downloaded 175 times

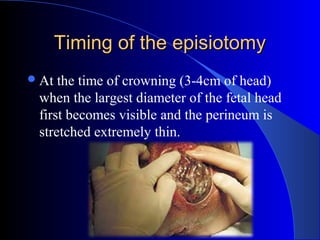


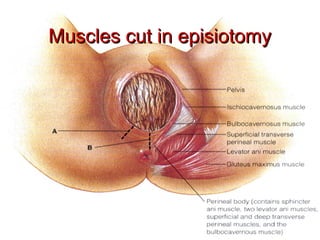
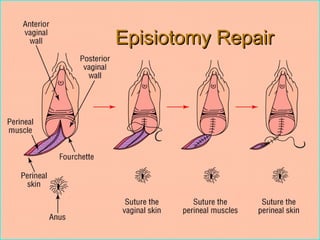


This document defines an episiotomy as a surgical incision made in the perineum and posterior vaginal wall during childbirth to enlarge the vaginal opening. It discusses the objectives, indications, timing, types, and steps for performing a mediolateral episiotomy. It also covers repairing the episiotomy, potential complications, and post-operative care recommendations such as applying ice, keeping the wound clean and dry, and encouraging sitz baths.
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

