Downloaded 673 times




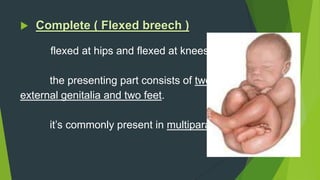








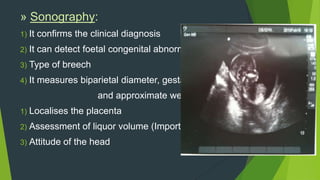


This document discusses breech presentation, which occurs when the fetus is in a longitudinal lie with the buttocks or feet presenting at the pelvic brim instead of the head. The incidence is about 3-4% and spontaneous correction usually occurs by 34 weeks. Breech presentations are classified as complete or incomplete. Etiologies include prematurity, factors preventing version, fetal abnormalities, and multiparity. Diagnosis involves clinical examination and sonography to determine type and position of breech.

















































![Breech presentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/breechpresentationautosaved-211128120250-thumbnail.jpg?width=640&height=640&fit=bounds)





