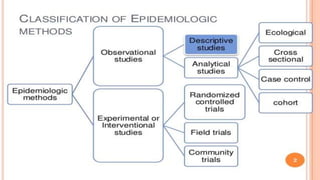
Epidemiology is defined as the study of the distribution and determinants of health-related states or events in populations and the application of this study to control health problems. It involves descriptive studies that ask questions about disease occurrence, magnitude, location, time period, and affected individuals. Analytical studies like case-control and cohort studies are used to test hypotheses about disease causes. Randomized controlled trials experimentally study interventions by applying or withdrawing suspected causes between study groups.