Download to read offline

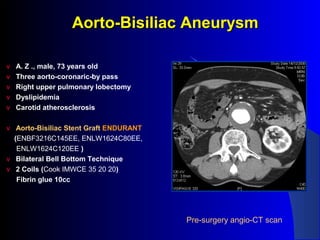
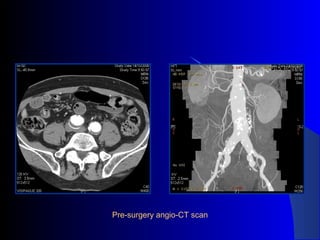

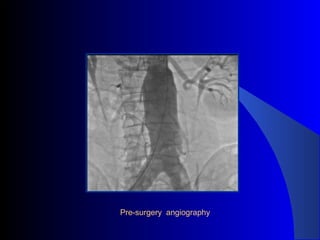
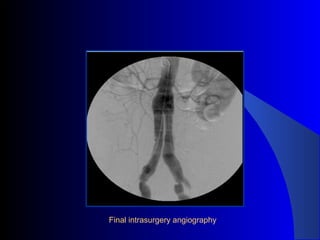
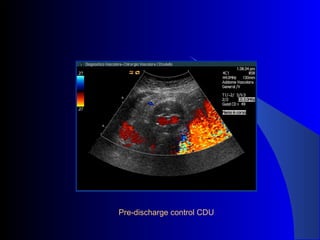


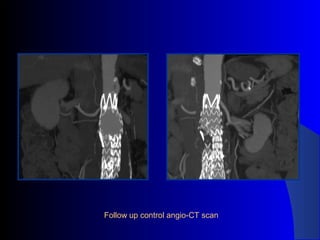

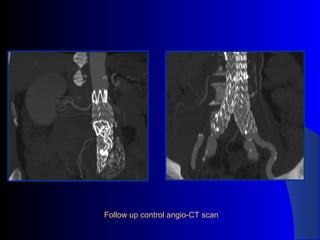


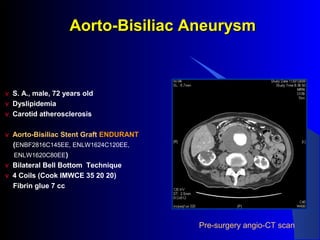

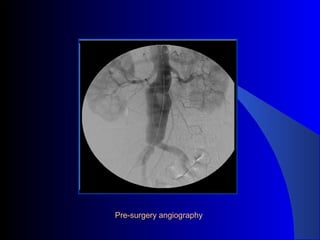

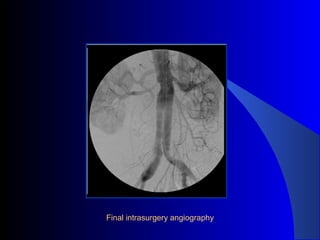



The document discusses the clinical application of the Endurant stent graft system in treating aorto-bisiliac aneurysms, detailing procedures performed on two male patients aged 72 and 73. Each patient had a history of dyslipidemia and carotid atherosclerosis, with procedures involving the bilateral bell bottom technique and the use of coils and fibrin glue. It includes pre-surgery imaging, intrasurgery angiography, and follow-up control scans to monitor outcomes.




























































































