Downloaded 458 times
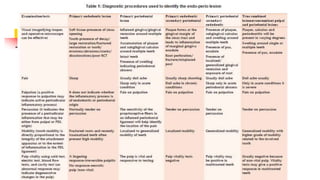



This document discusses periodontal-endodontic lesions, including: - The relationship between the periodontium and pulp and pathways of communication between them. - Classifications of lesions based on origin as primary endodontic, periodontal, or combined. - Diagnosis involves determining the origin of the lesion and ruling out other causes. - Treatment depends on the classification but generally involves endodontic treatment, periodontal treatment, or both to fully resolve the lesion. Prognosis depends on the extent and chronicity of the periodontal involvement.






























































![endo-perio_inter_relationship__perio_[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/endo-periointerrelationshipperio1-241130141949-61d8dbcb-thumbnail.jpg?width=640&height=640&fit=bounds)





















