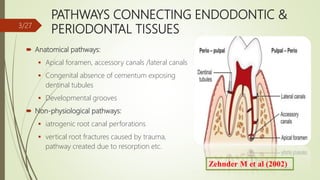
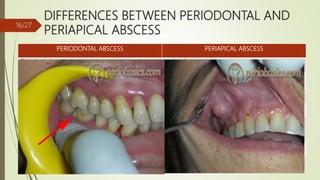
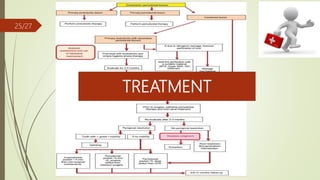
This document discusses the relationship between endodontic and periodontal tissues. It begins by introducing endo-perio lesions and noting they are responsible for over 50% of tooth mortality. It then covers pathways connecting endodontic and periodontal tissues, the etiology and classification of endo-perio lesions, diagnostic procedures, differences between periodontal and periapical abscesses, the endo-perio controversy, and treatment approaches. The document provides an overview of the interactions between the endodontic and periodontal systems and debates around their relationships.













































![endo-perio_inter_relationship__perio_[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/endo-periointerrelationshipperio1-241130141949-61d8dbcb-thumbnail.jpg?width=640&height=640&fit=bounds)


































