This document discusses endodontic radiography and the importance of radiographs in endodontic diagnosis and treatment. It provides a brief history of radiography and describes common types of radiographs used in endodontics like intraoral periapical radiographs and cone beam computed tomography (CBCT). Intraoral periapical radiographs allow visualization of the root structure and surrounding bone. CBCT provides high quality 3D images with less radiation compared to traditional CT. The document emphasizes that radiographs are essential for endodontic diagnosis, treatment planning, working length determination, and follow-up care.
![INTERPRETATION OF RADIOGRAPH
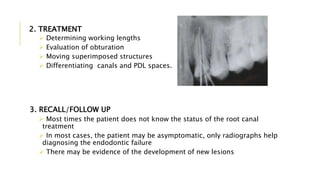
ACCORDING TO APPEARANCE
APPERANCE TENTATIVE FINDINGS
Black/Gray area a) Decay
b) Pulp
c) Gingiva or space between teeth
d) Abscess
e) Cyst
White area a) Enamel
b) Restoration [ metal, gutta percha,
etc. ]
Creamy white area Dentin appears as creamy white area
White line around teeth Lamina dura around teeth](https://image.slidesharecdn.com/endodonticradiography-201217093927/85/Endodontic-Radiography-5-320.jpg)
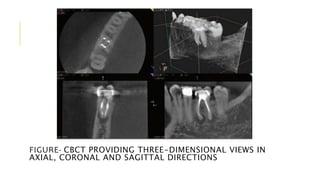
![CONE BEAM COMPUTED
TOMOGRAPHY
It’s a diagnostic imaging modality that provides high quality,
accurate three-dimensional representation of the osseous
elements of the maxillofacial skeleton
It is a form of computed tomography in which only a focused,
cone-shaped beam of X-ray is projected at the imaged tissue
The limited volume significantly reduces the amount of
radiation compared with traditional computed tomography
The resolution of the CBCT image is low, which allows
visualization of very small objects, such as difficult to find
canals [pixels resolution ranging from 0.4 mm to 0.076 mm]](https://image.slidesharecdn.com/endodonticradiography-201217093927/85/Endodontic-Radiography-13-320.jpg)