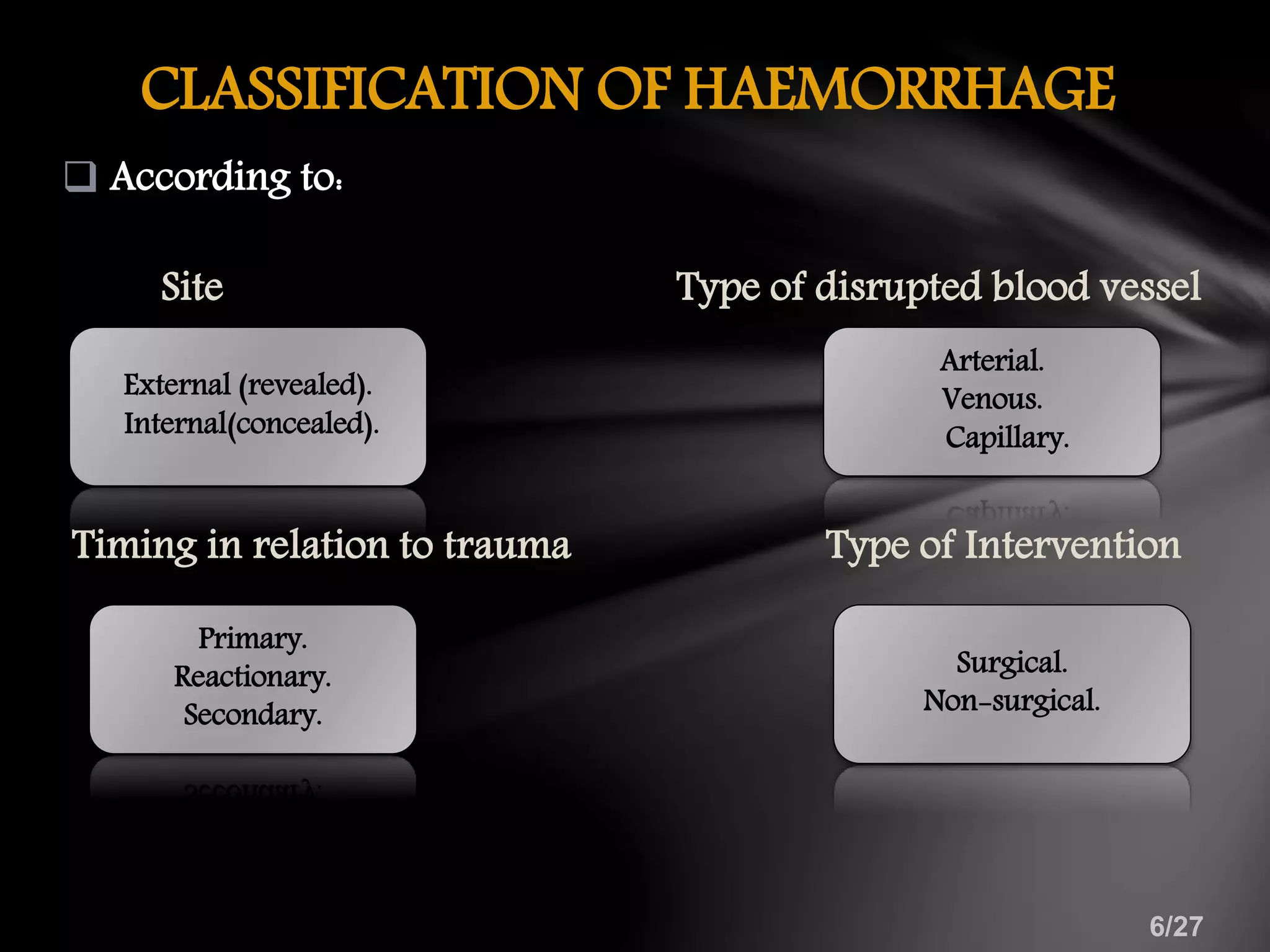
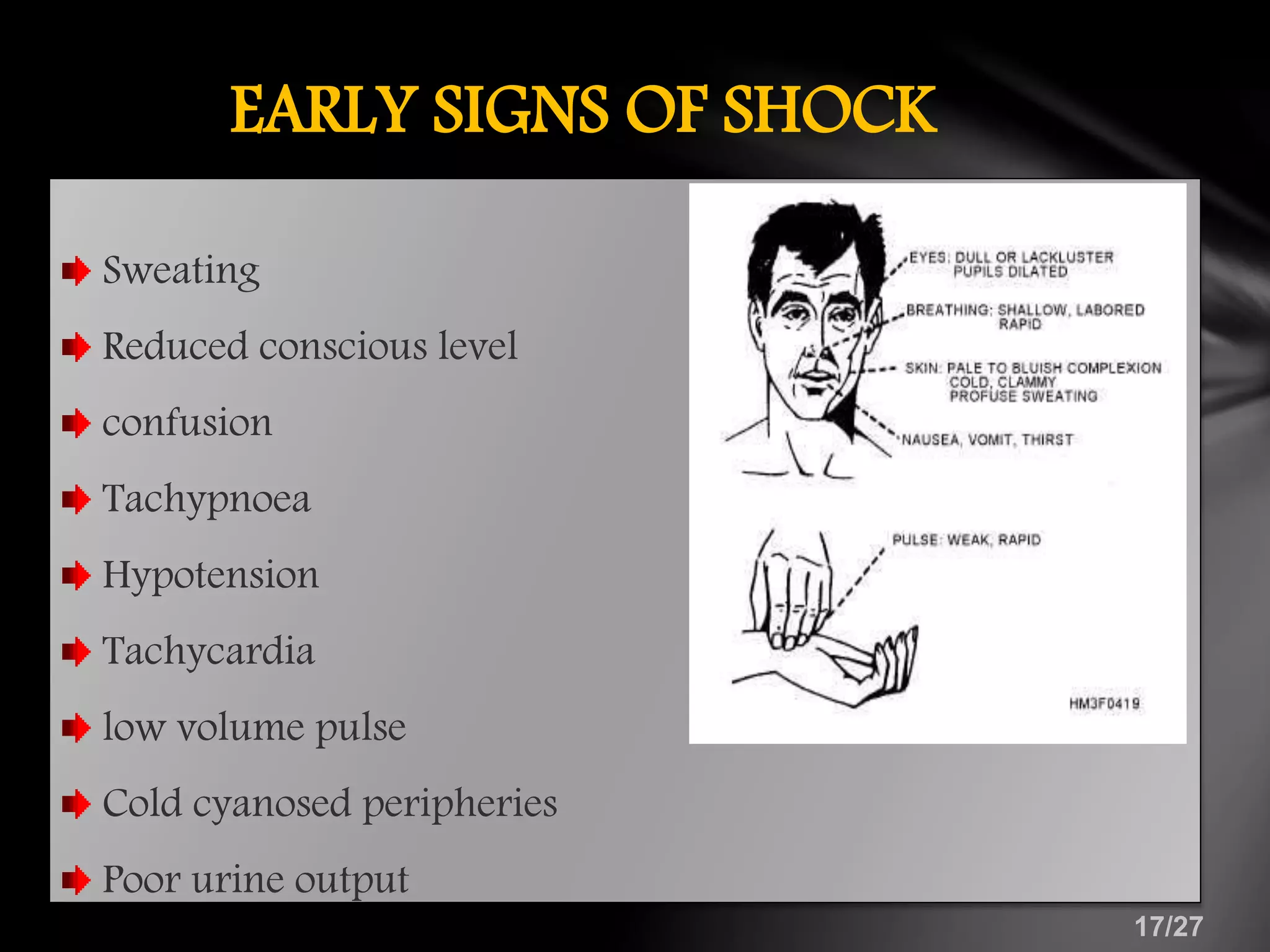
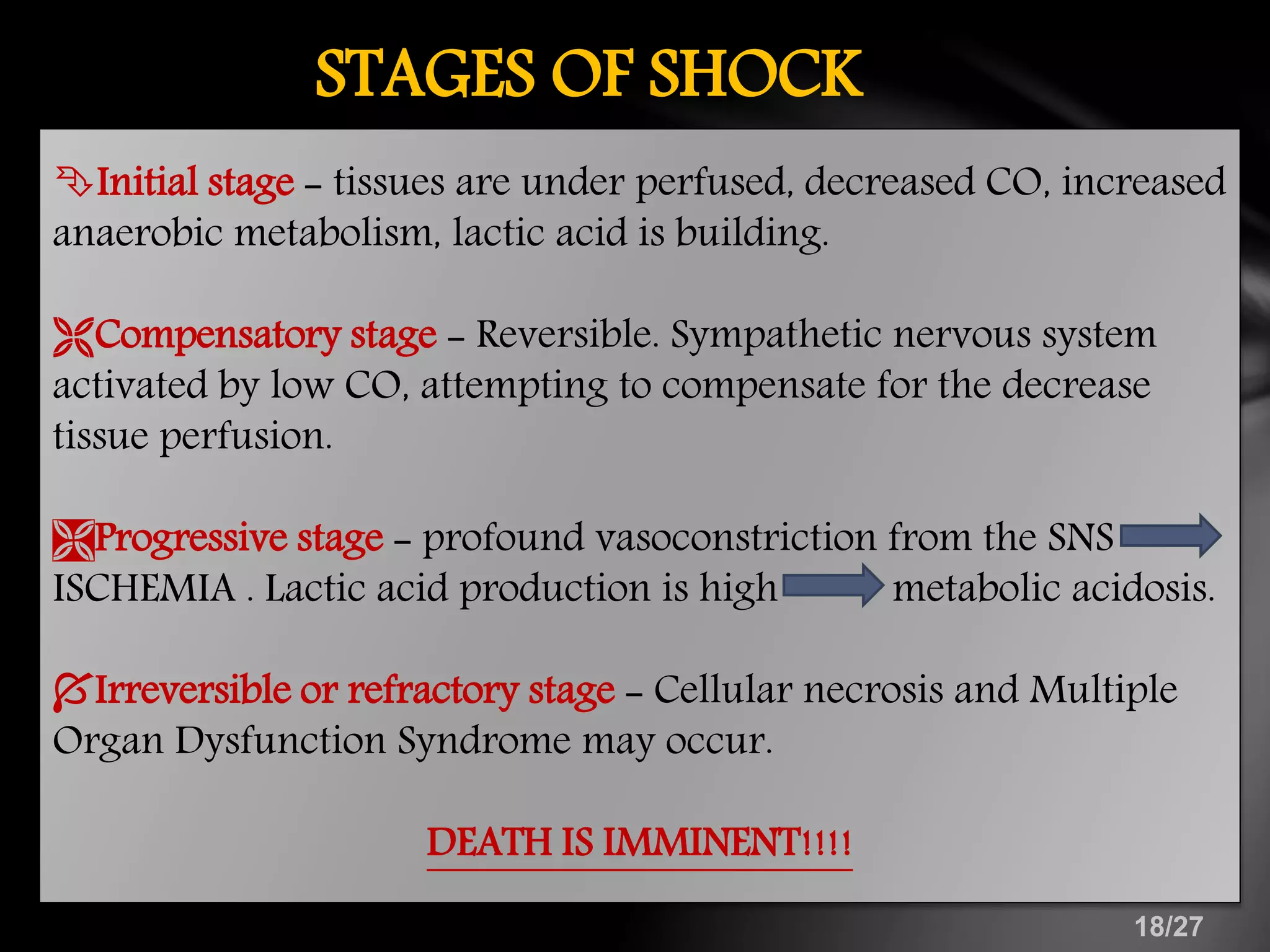
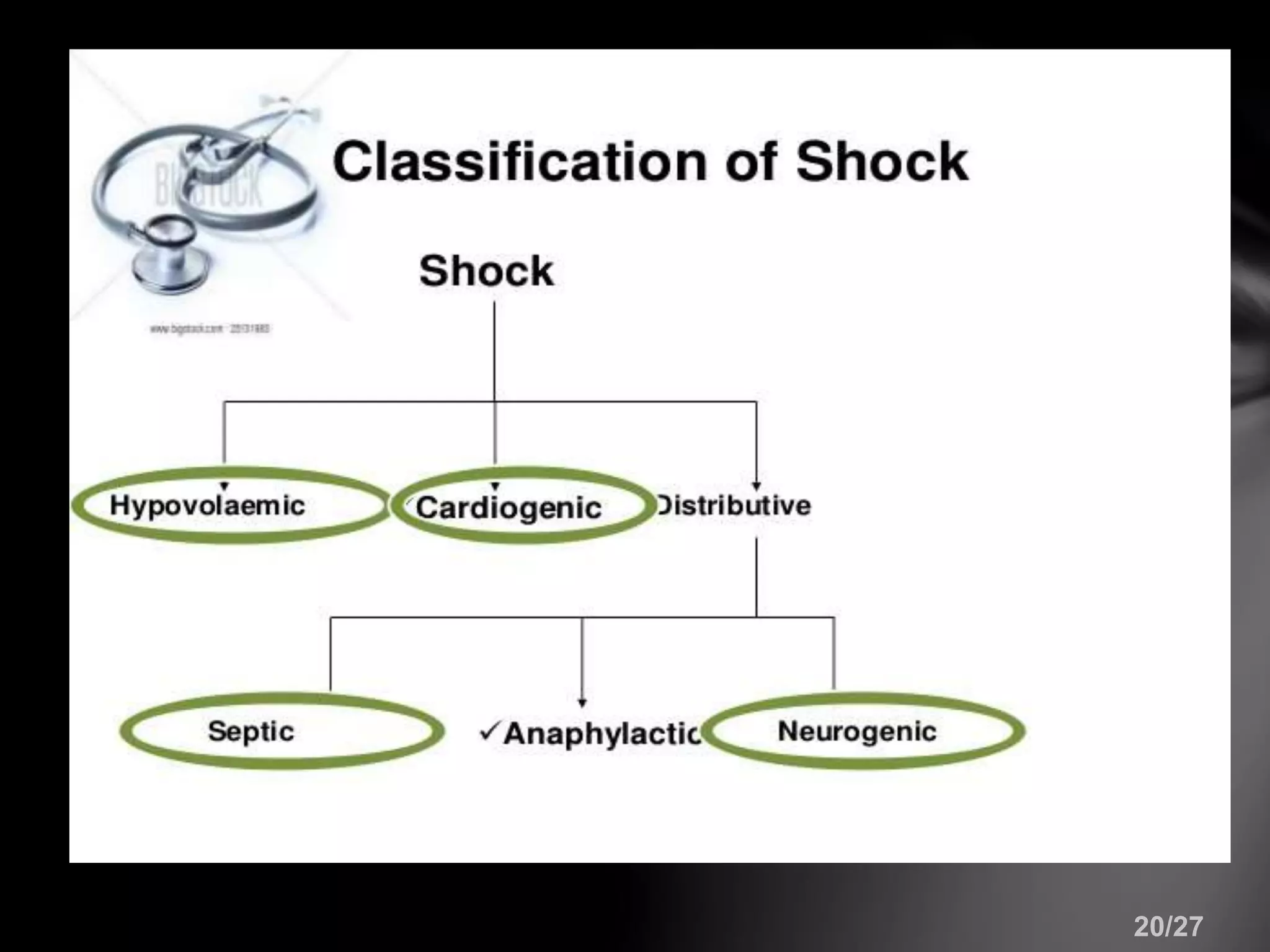
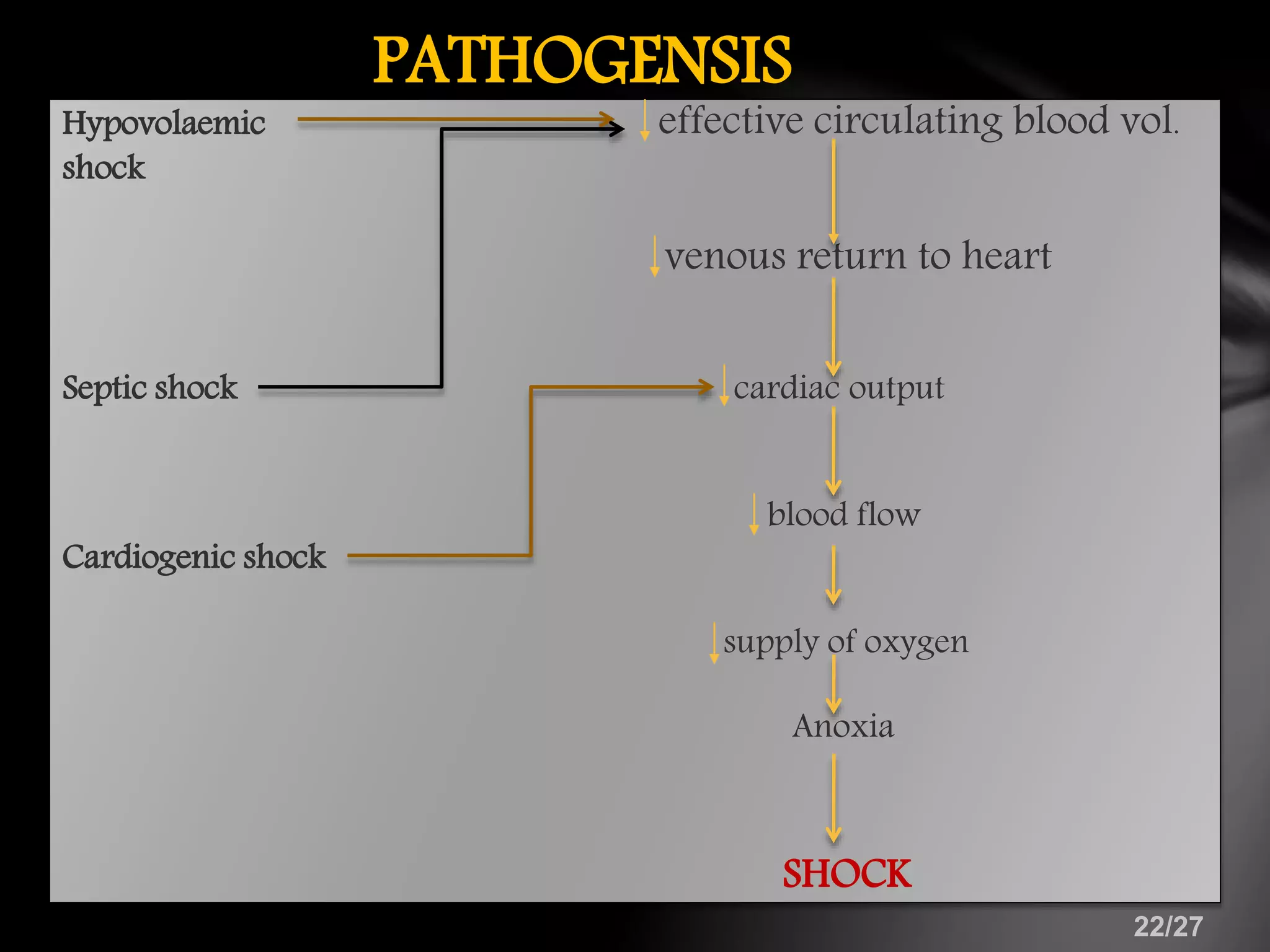
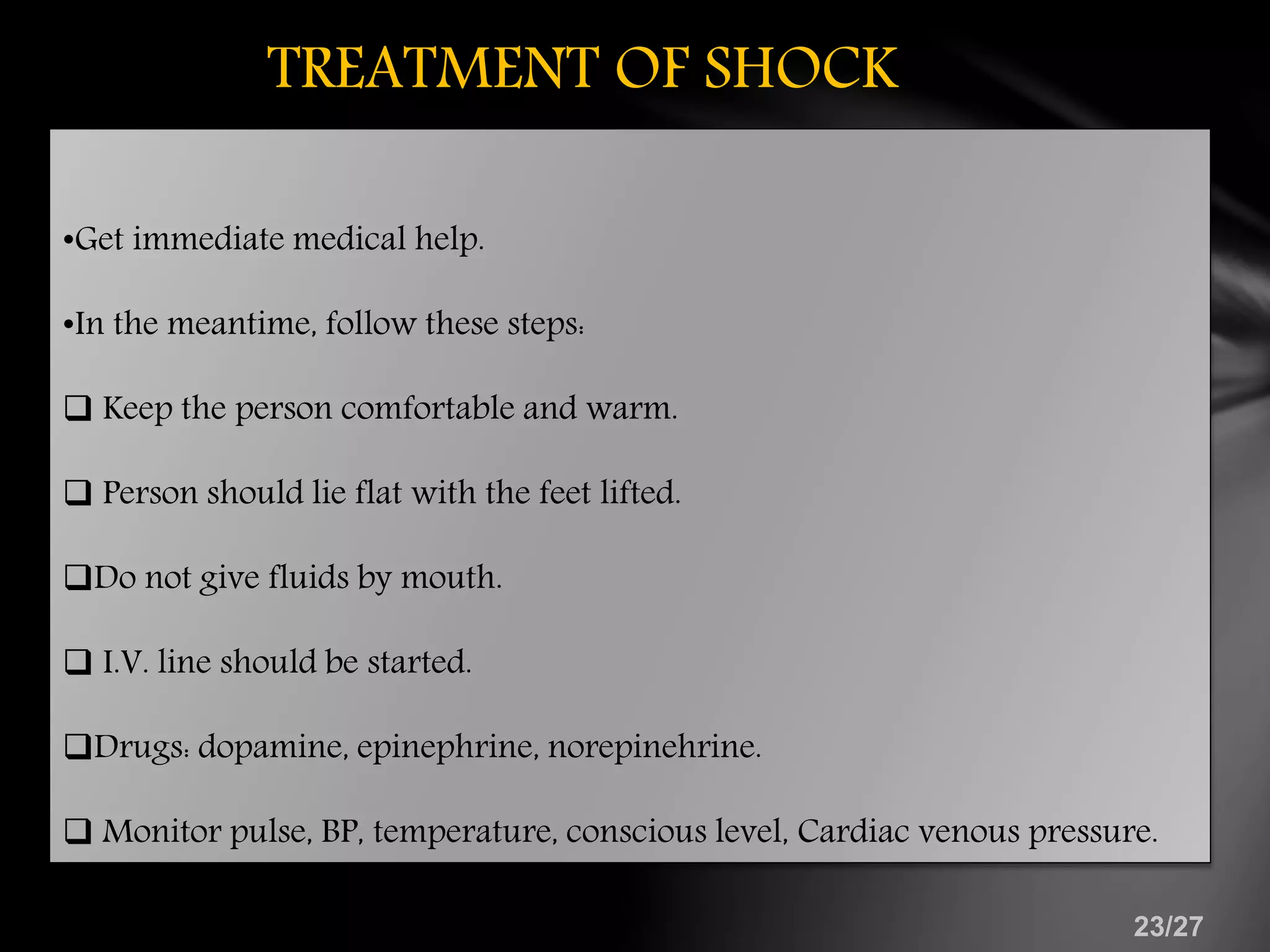
This document discusses haemorrhage and shock. It defines haemorrhage as bleeding from damaged blood vessels, and classifies it based on site, vessel type, timing, and intervention needed. Shock is defined as insufficient oxygen delivery to tissues. The document outlines signs of haemorrhage and shock, degrees of blood loss, measurement methods, and management approaches including fluid resuscitation and hemostatic measures. It also describes types of shock including hypovolemic, septic and cardiogenic shock, and their pathogenesis. Treatment of shock focuses on stabilization, IV fluids, and vasopressor drugs. Complications in organs like heart, lungs, and liver are also summarized.























































![shock and Hemorrhage. ppt [ janvi ]](https://cdn.slidesharecdn.com/ss_thumbnails/janvishockandhemorrhage-240926160708-481056f0-thumbnail.jpg?width=640&height=640&fit=bounds)










































