Downloaded 145 times

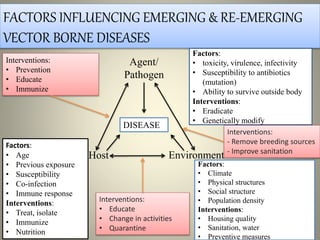
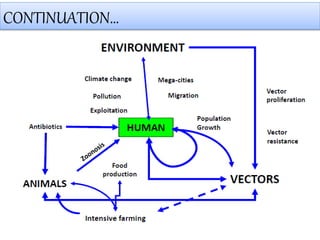



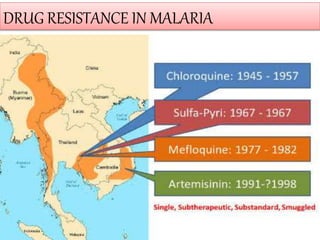



The document provides an overview of emerging and re-emerging vector-borne diseases, detailing factors influencing their prevalence and methods for control and prevention. It highlights the complex interactions between pathogens, hosts, and environments, as well as the importance of surveillance, response strategies, and international collaboration. The Integrated Disease Surveillance Project (IDSP) and International Health Regulations (IHR) are discussed as frameworks for managing public health threats globally.



































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)