Downloaded 383 times
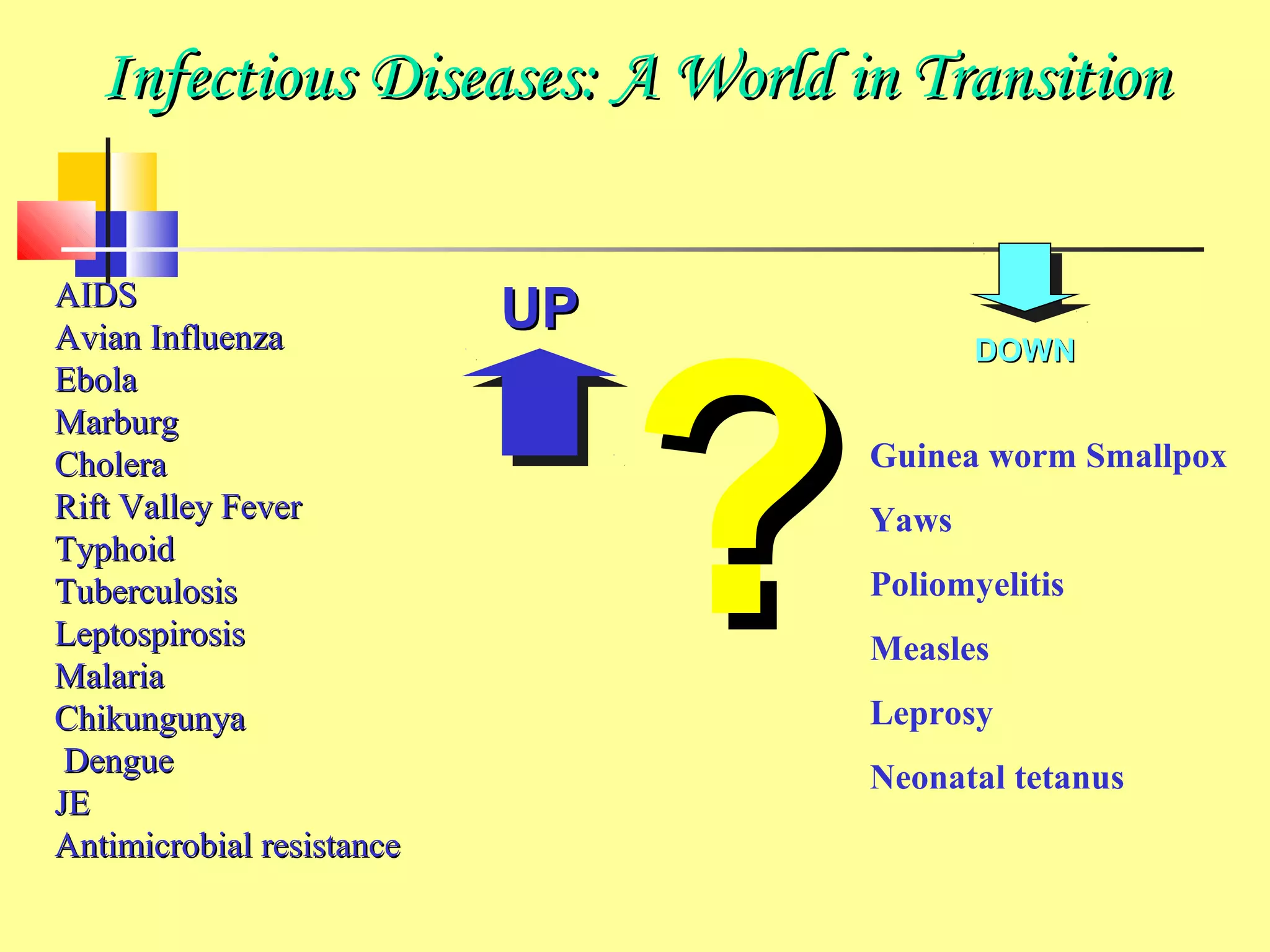
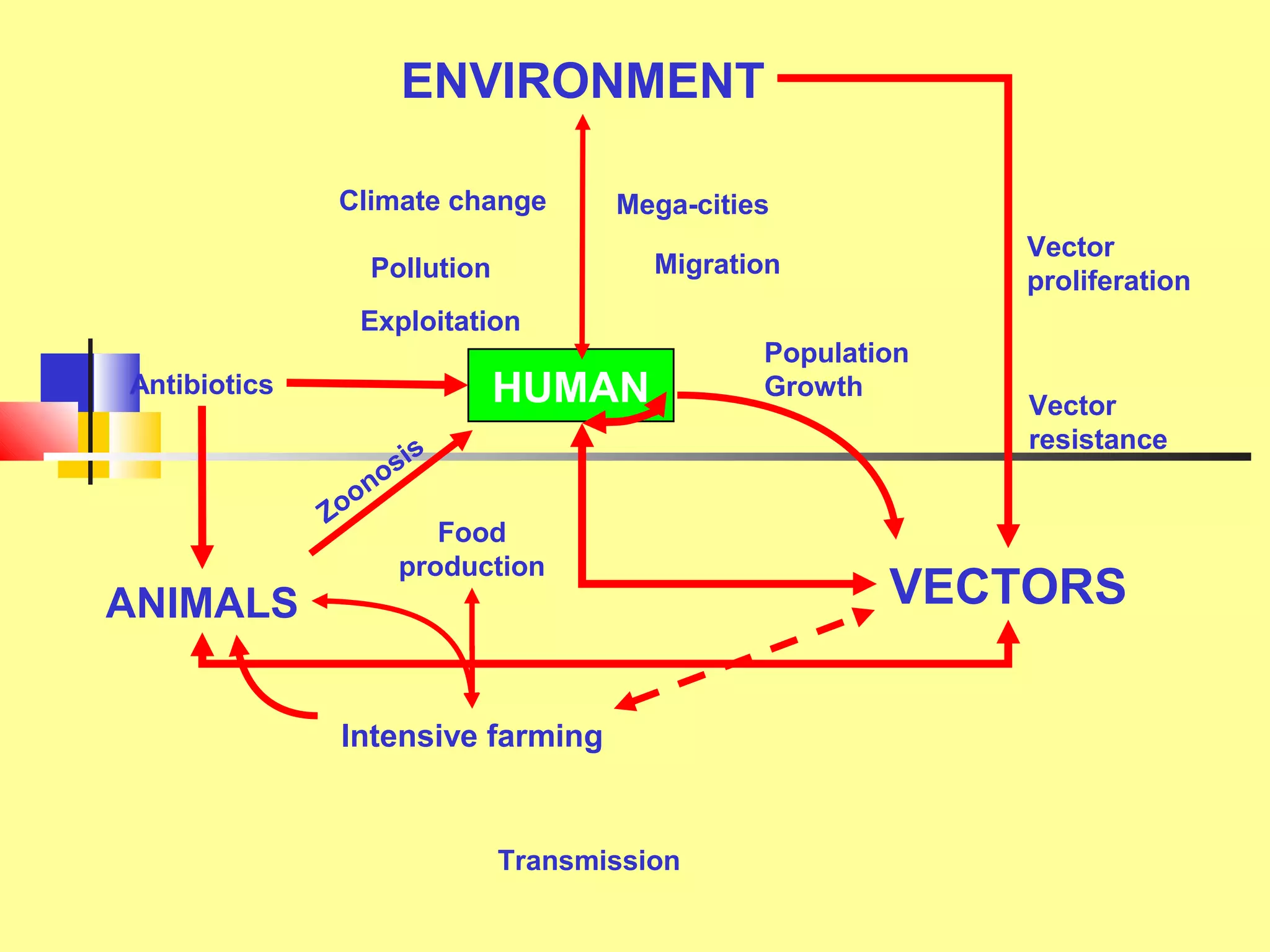
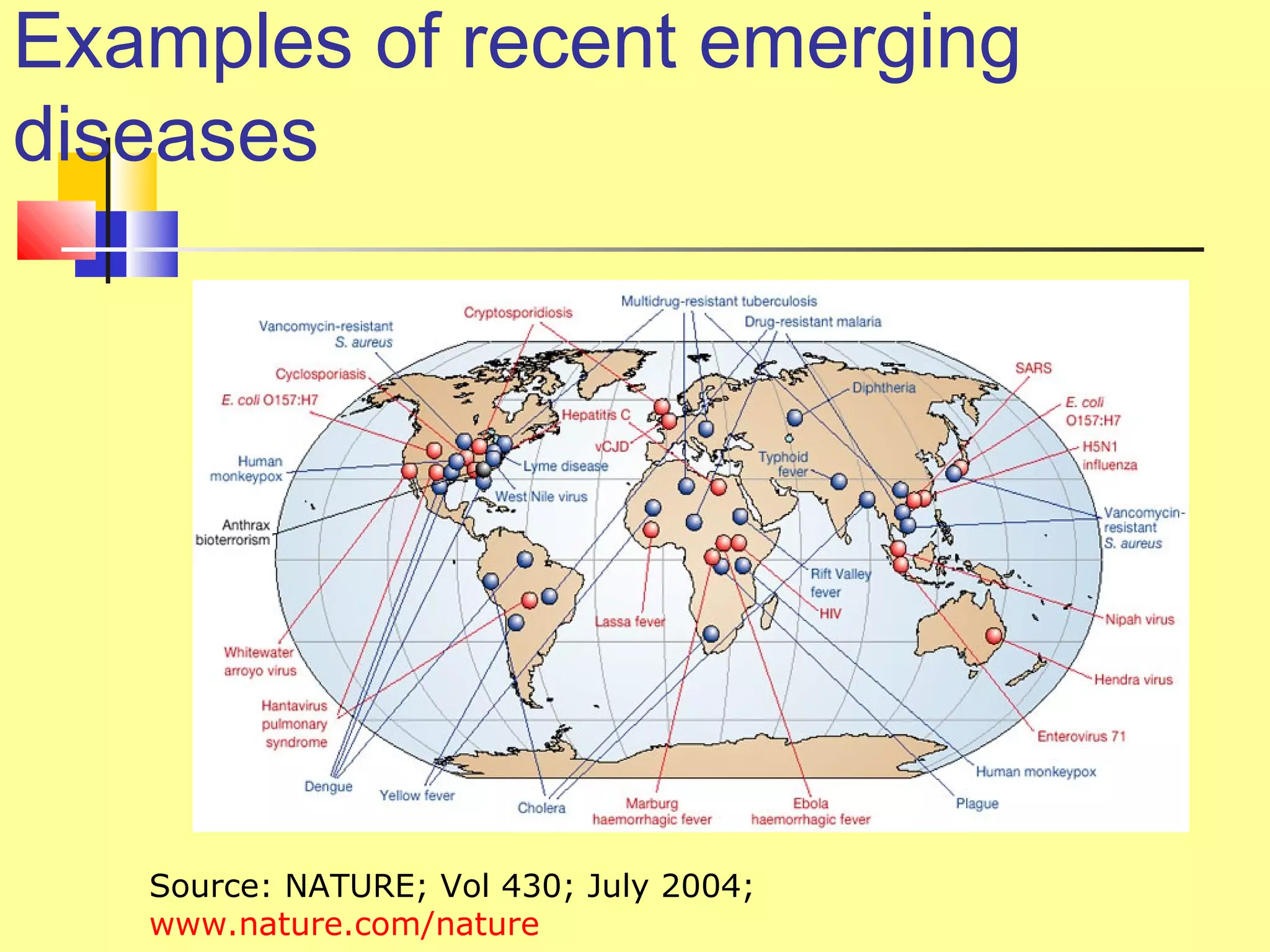
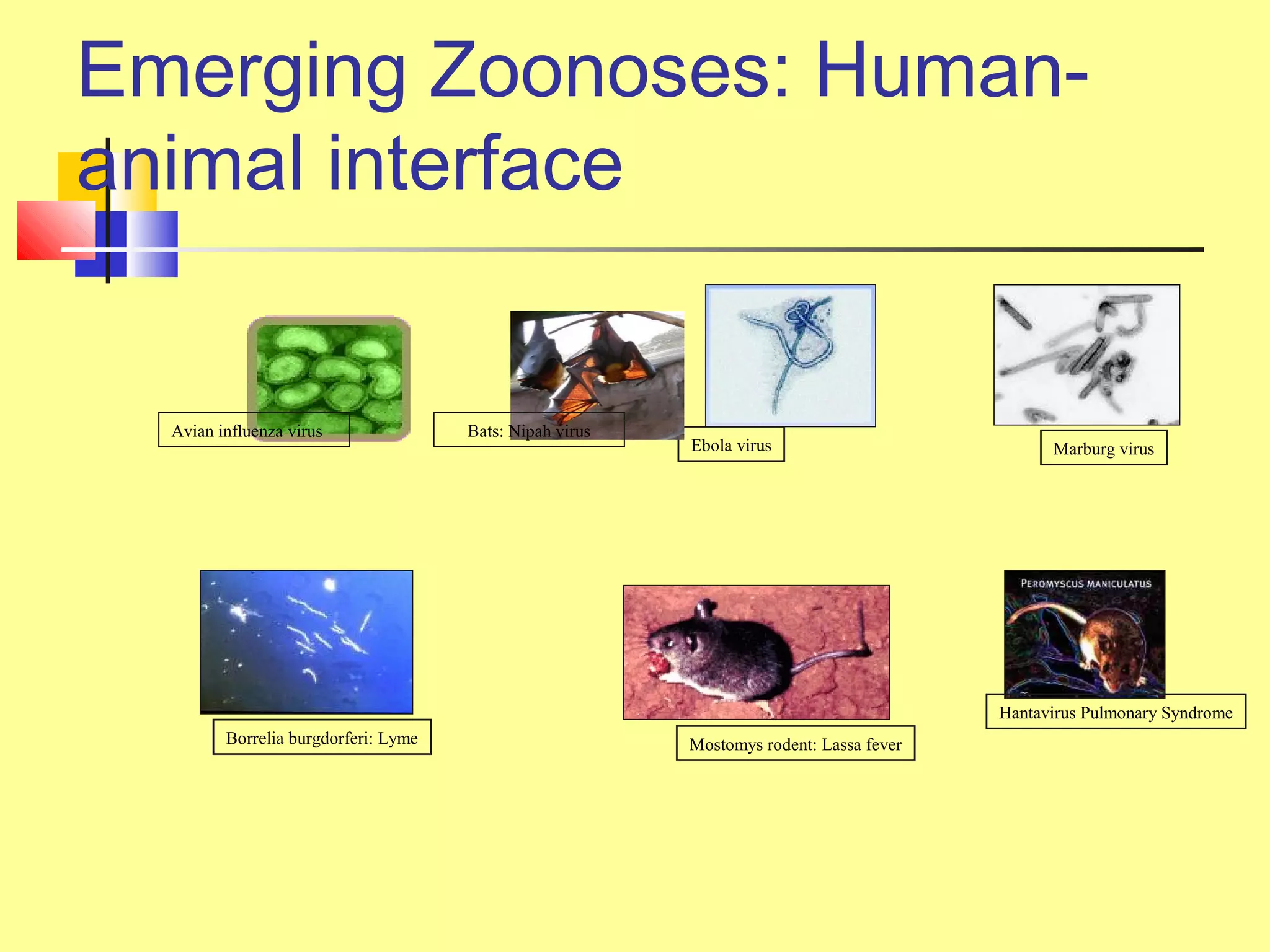
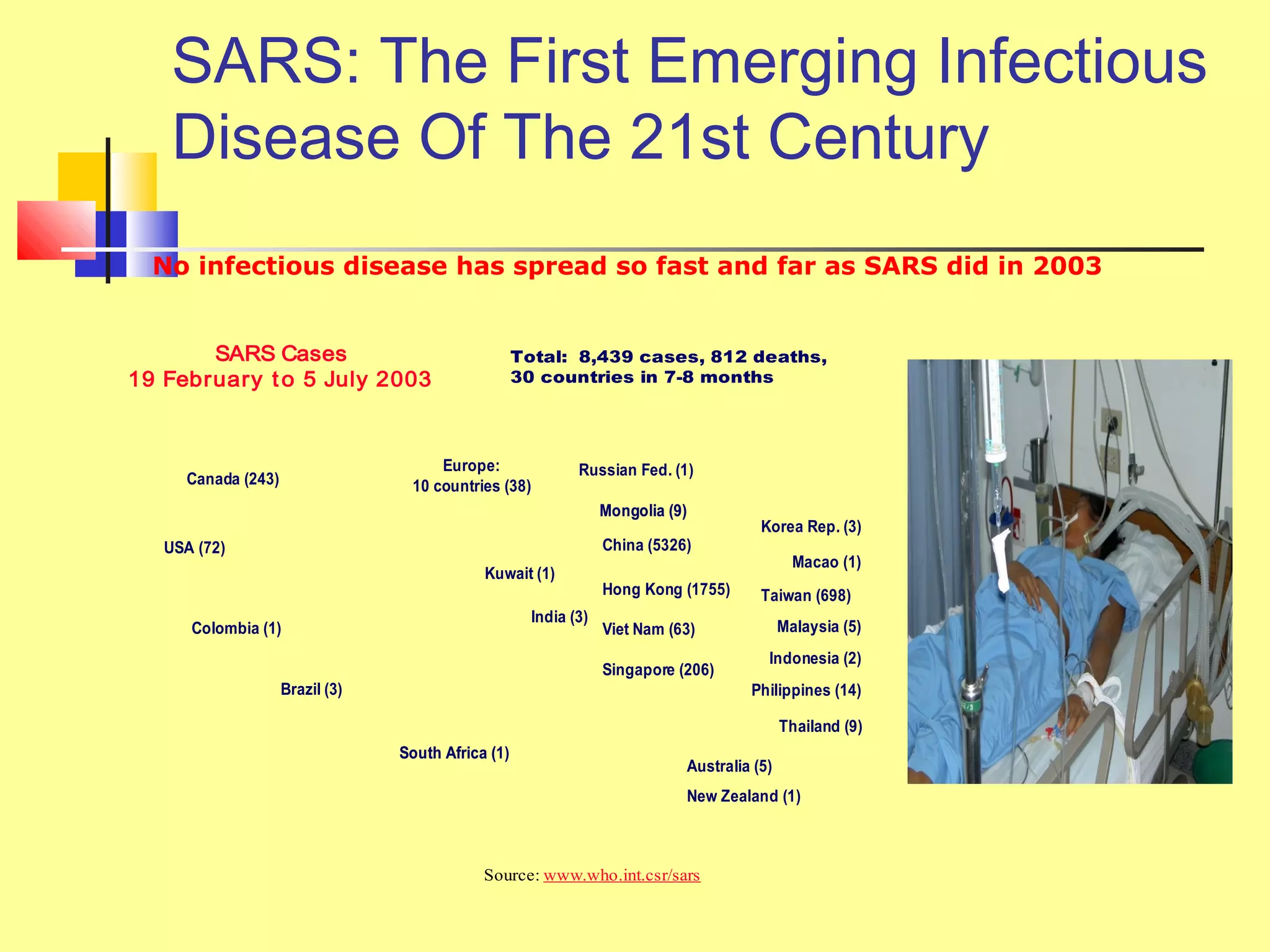



This document provides an overview of emerging and re-emerging infectious diseases. It discusses trends showing a resurgence of infectious diseases since the late 20th century. Emerging diseases are newly identified agents causing health issues, while re-emerging diseases were previously controlled but are increasing. Factors driving emergence include changes in human, animal and environmental conditions. Examples are given of recent emerging diseases like SARS, avian influenza, and drug-resistant pathogens. National surveillance and global cooperation are needed to monitor, investigate and respond to infectious disease threats.



































































