Downloaded 21 times
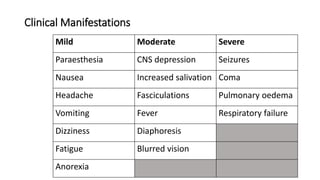

The document discusses insecticides, their types, and their potential toxicity to human health through various exposure routes, including inhalation, dermal contact, ingestion, and injection. It outlines both acute and chronic toxicity, as well as specific symptoms and clinical manifestations from different classes of insecticides, such as organophosphates and pyrethroids. The document emphasizes the importance of safety measures, proper handling, and treatment protocols for pesticide exposure and poisoning.