Downloaded 105 times


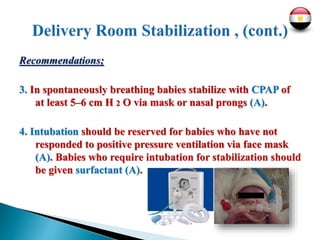



Three key interventions are recommended for managing respiratory distress syndrome (RDS) in preterm infants: 1. Administering a single course of prenatal corticosteroids to mothers at risk of preterm delivery between 23-34 weeks gestation to reduce the risk of RDS. 2. Stabilizing infants immediately after birth using controlled CPAP with supplemental oxygen, aiming for gradual increase in oxygen saturation levels. 3. Giving a natural surfactant preparation to infants with or at high risk of RDS, with early administration improving outcomes. The "INSURE" technique of administering surfactant via brief intubation can reduce need for mechanical ventilation.


















![National programs dr jason [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/nationalprograms-drjasonautosaved-210917011725-thumbnail.jpg?width=640&height=640&fit=bounds)










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










