Download to read offline


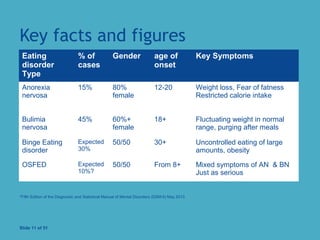
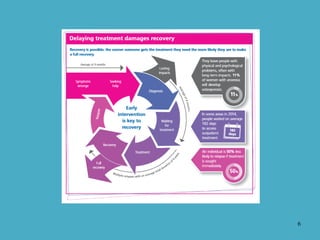

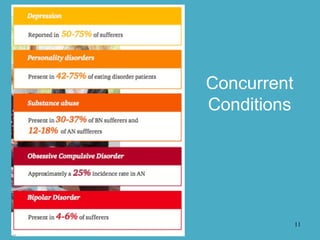
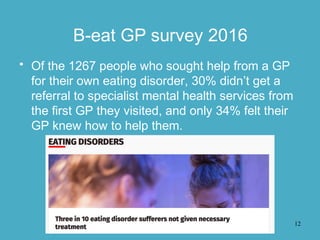
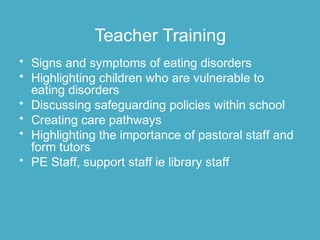





The document discusses early intervention strategies for eating disorders in schools, including assessments, training for staff, and family liaison. It highlights key statistics on the prevalence and onset of various eating disorders, noting that early treatment leads to significantly better outcomes. The document also emphasizes the importance of collaborative efforts among schools, parents, and healthcare providers in recognizing symptoms and facilitating timely referrals.


















































































