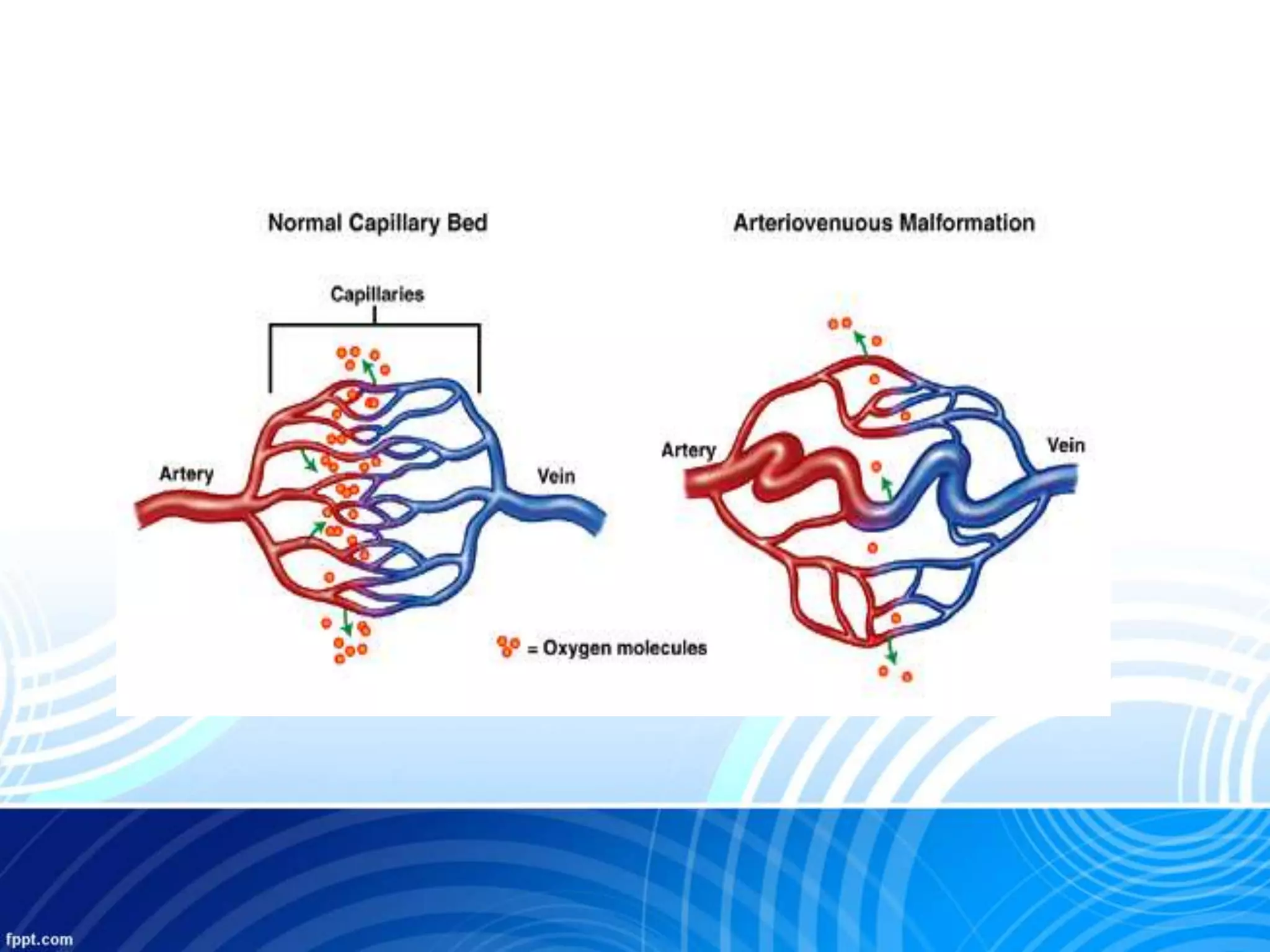
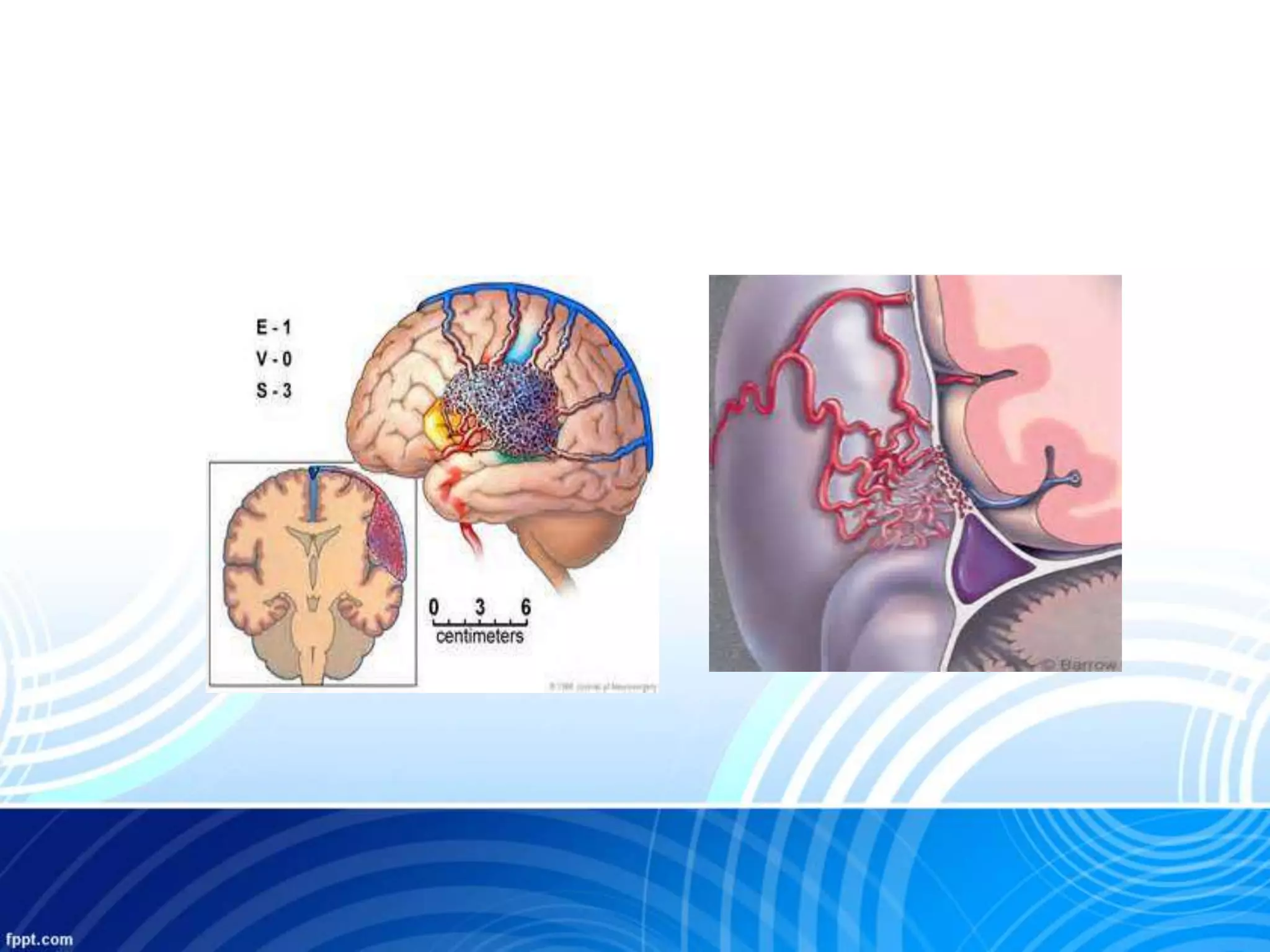
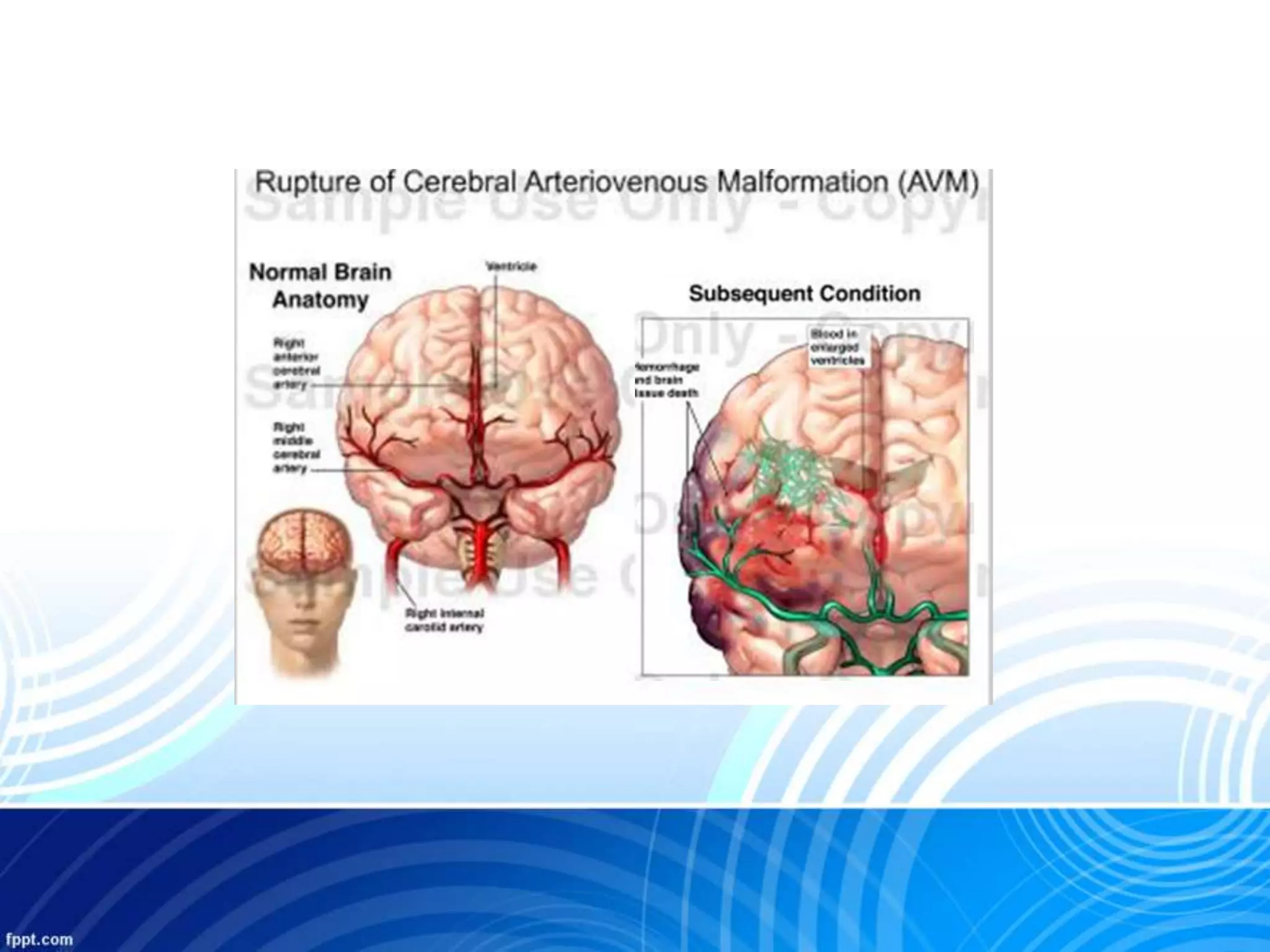
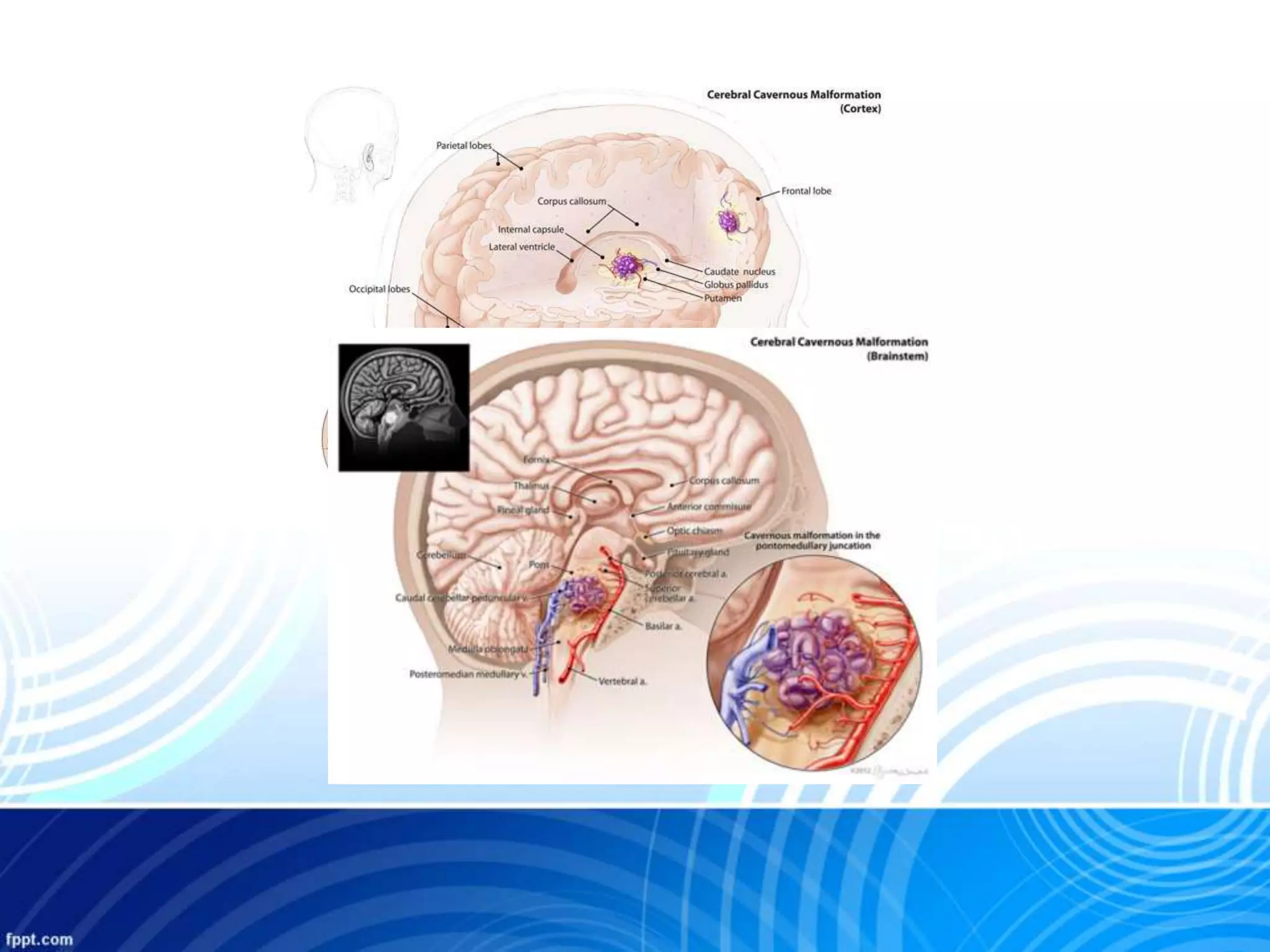
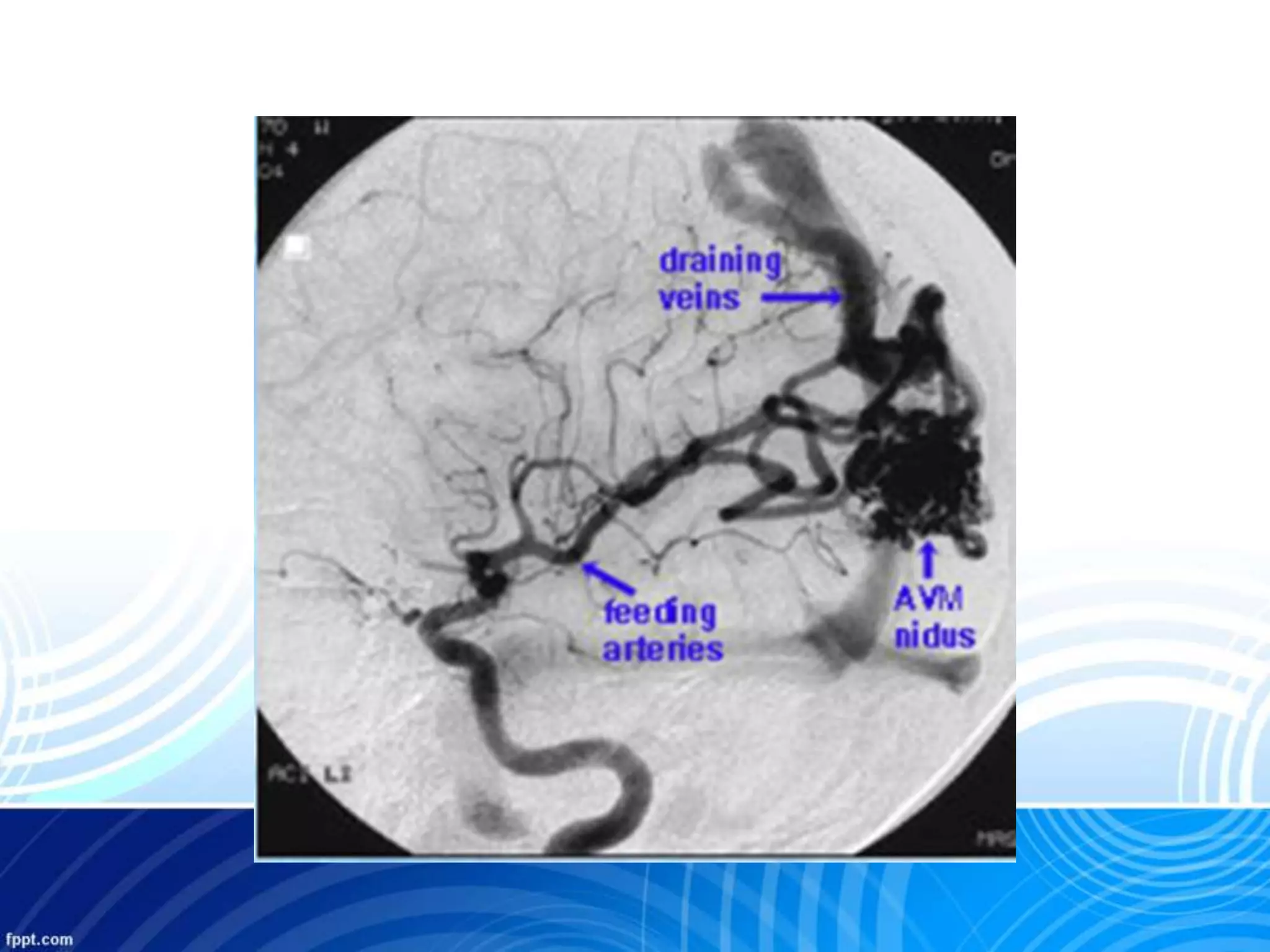
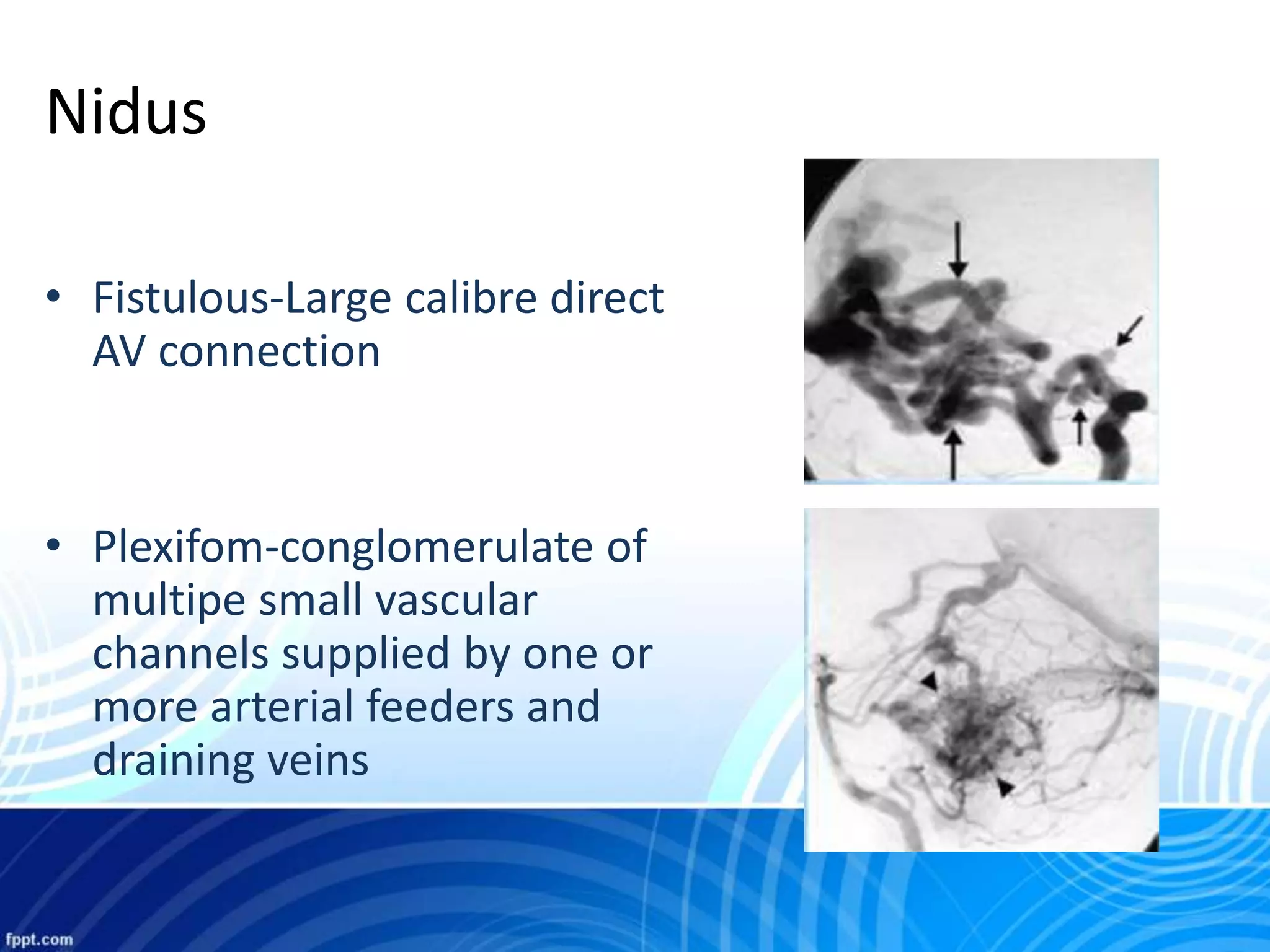
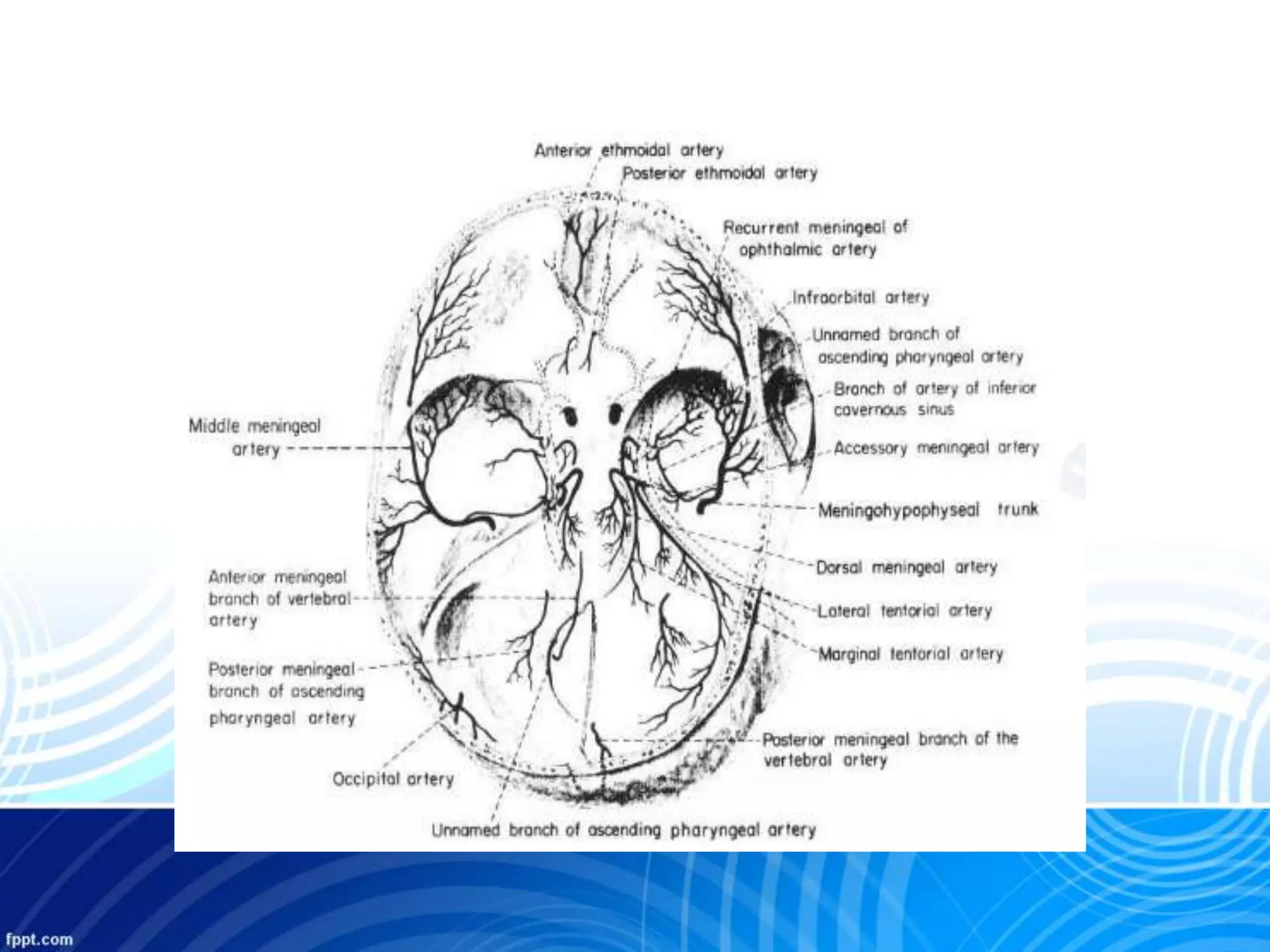
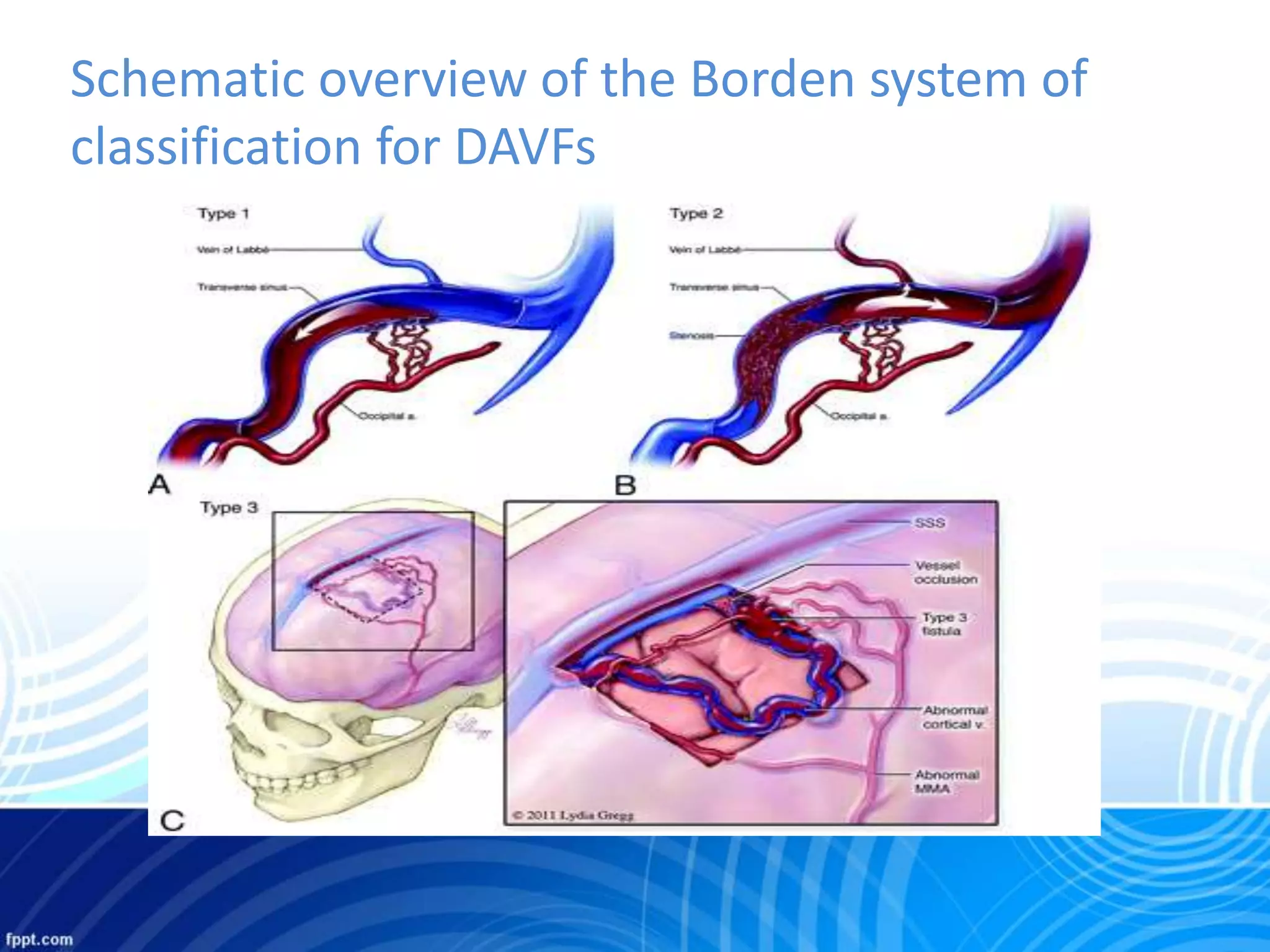
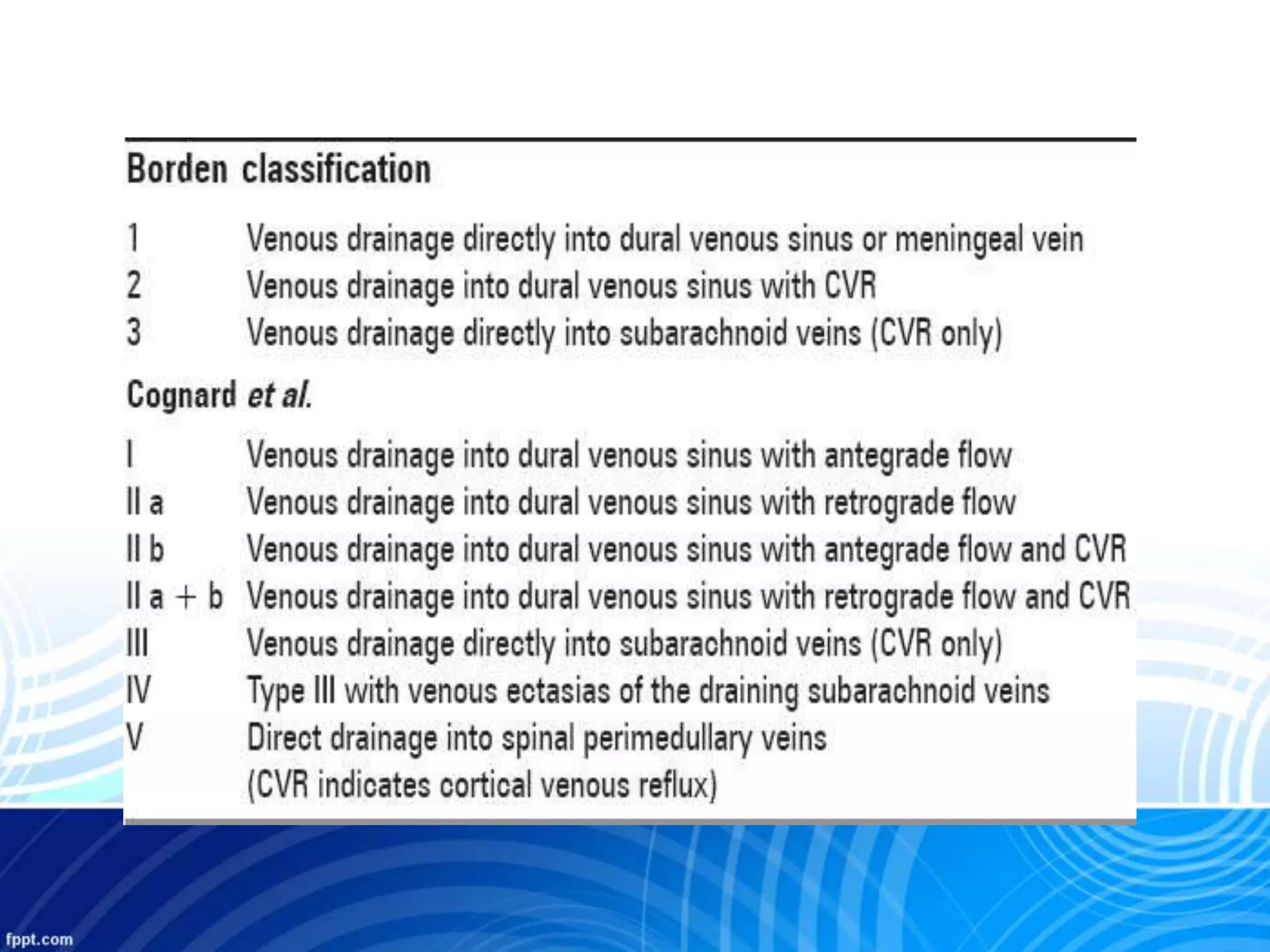
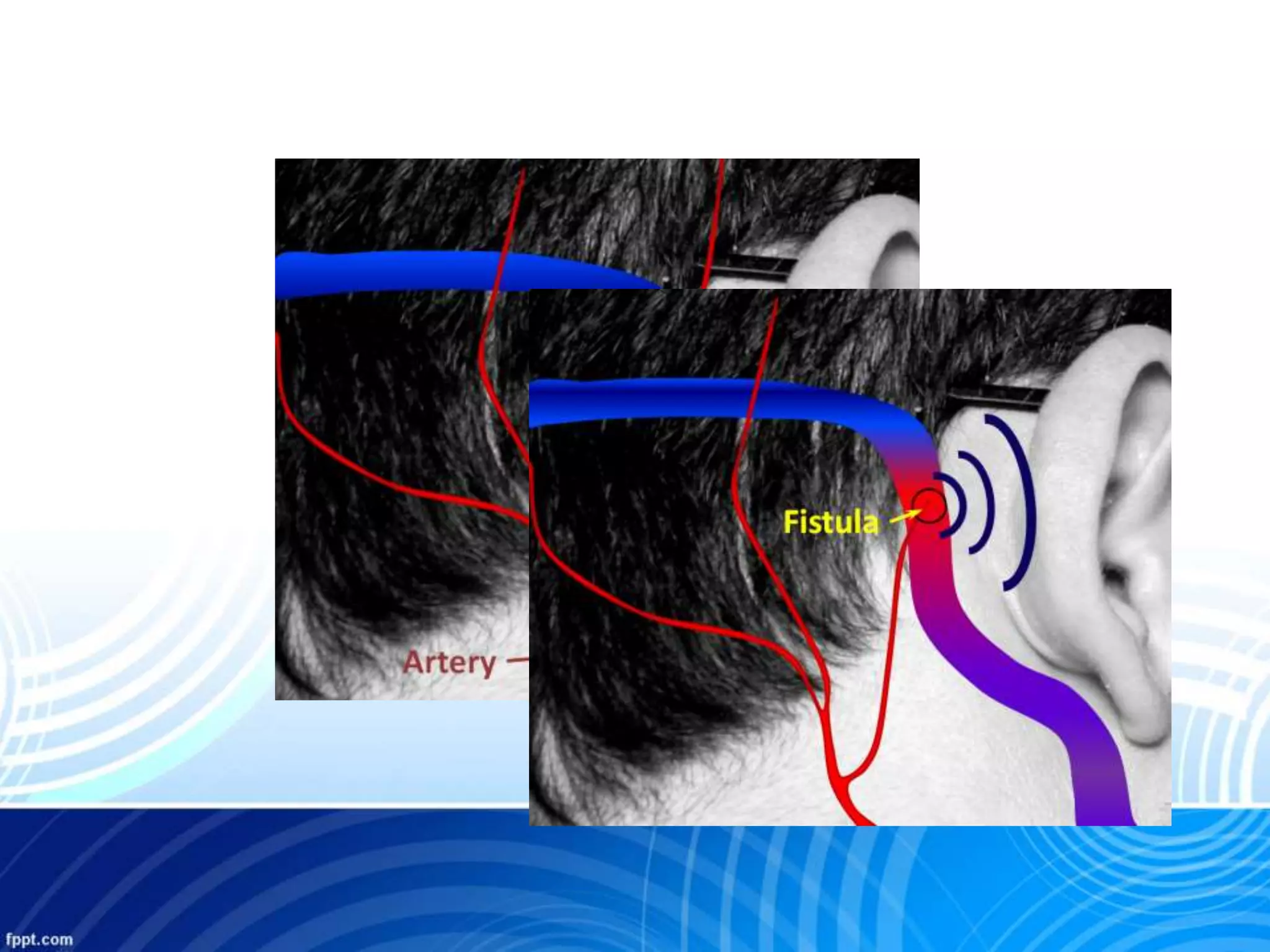
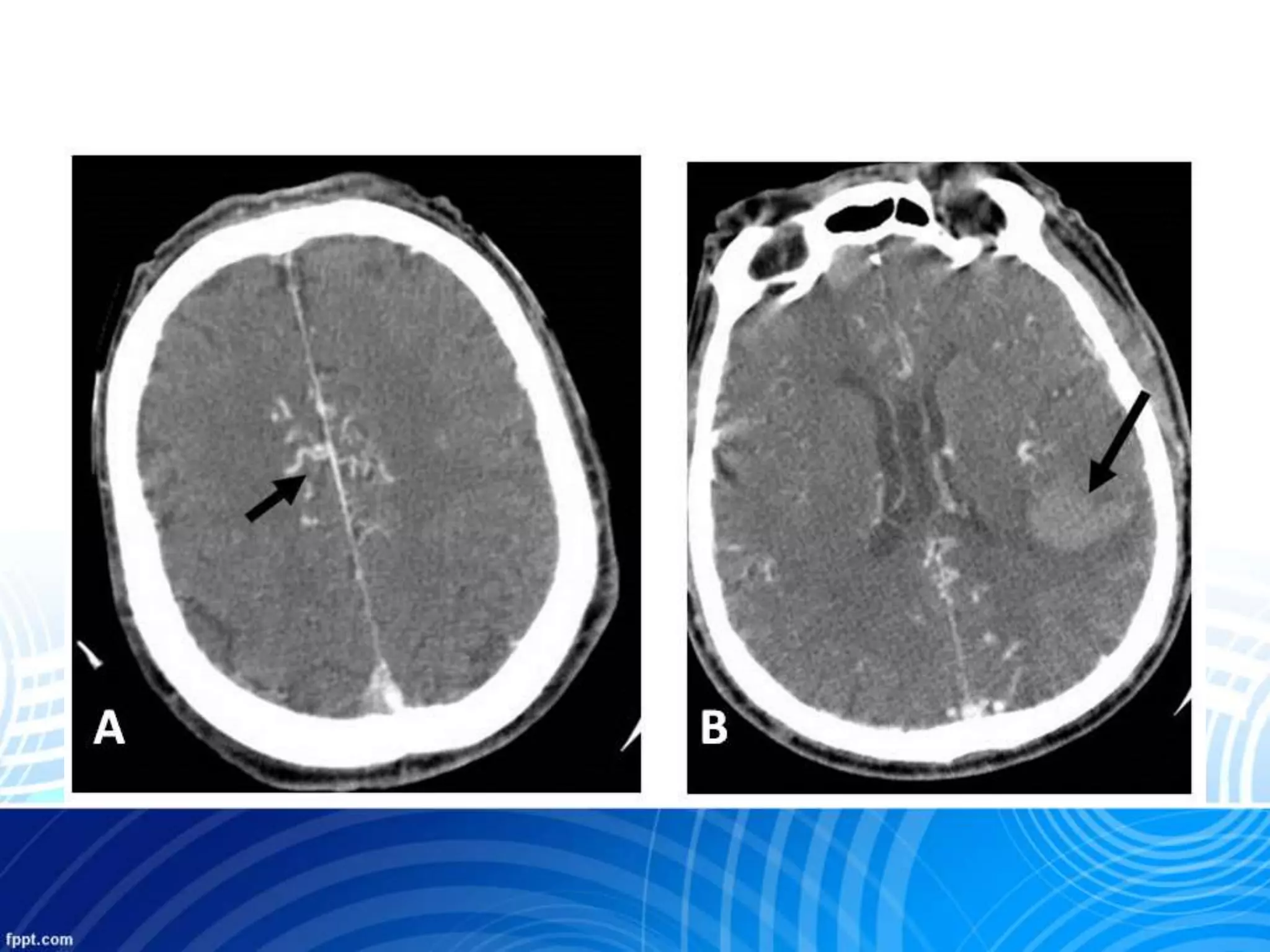
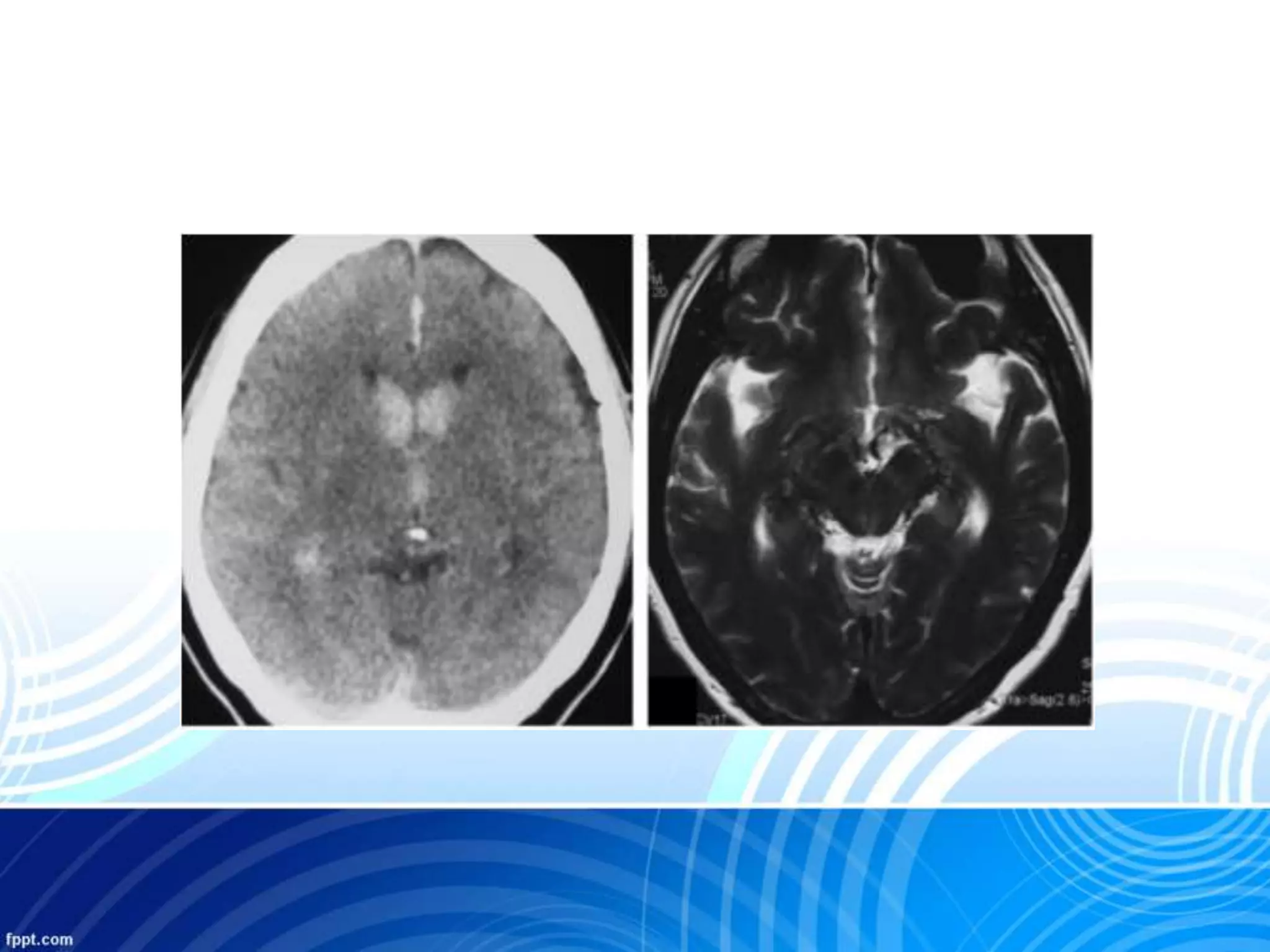
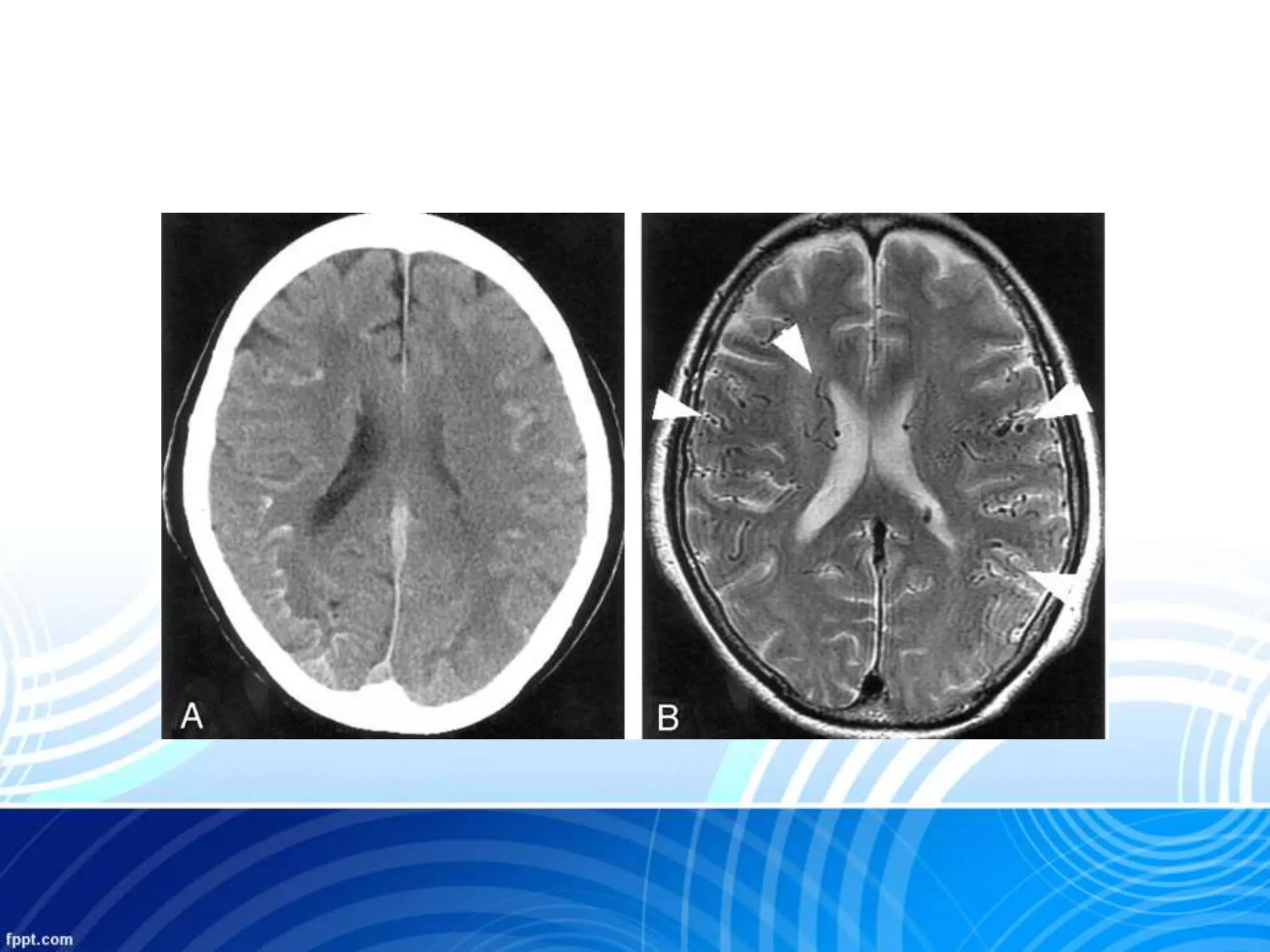
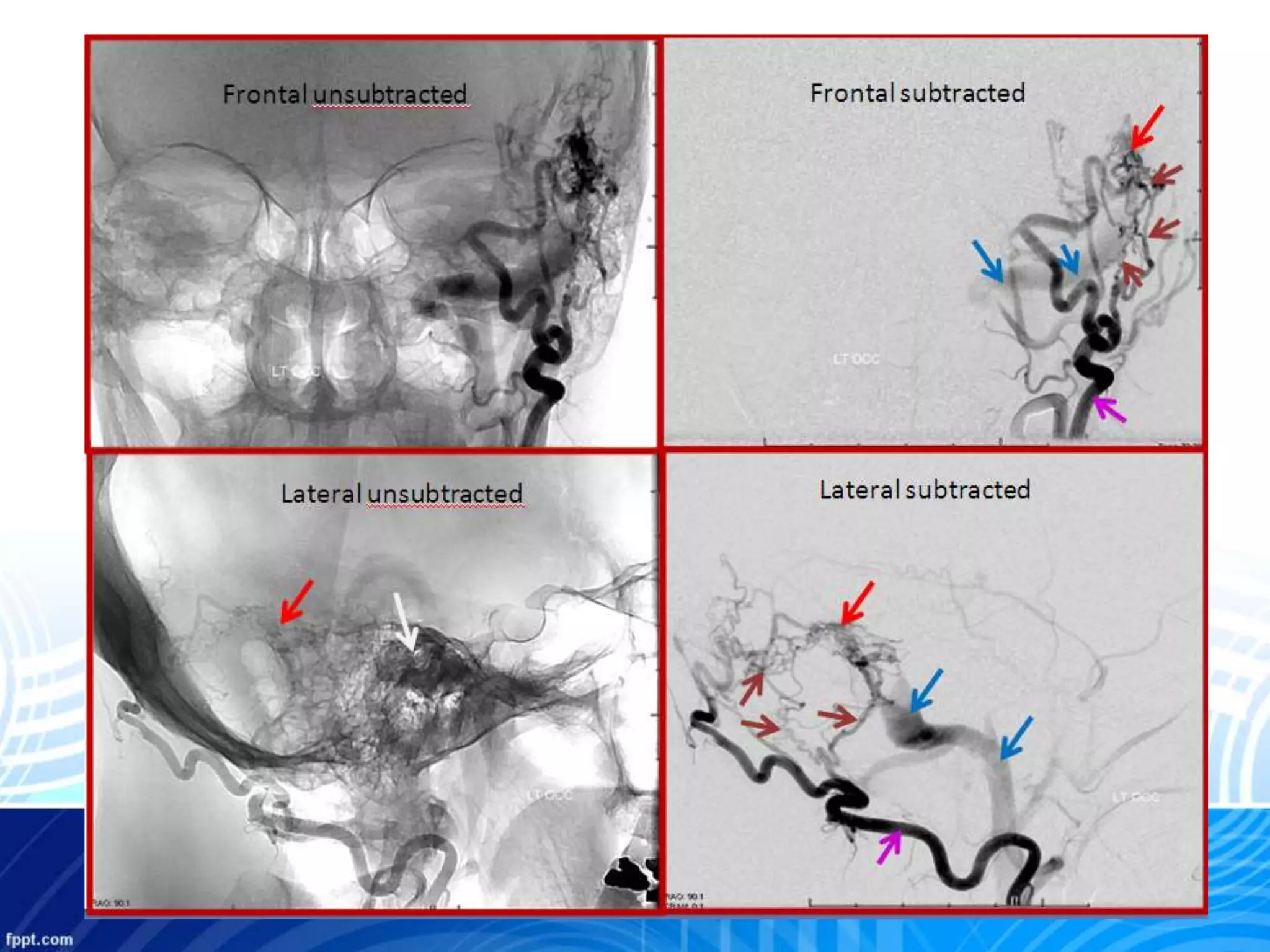
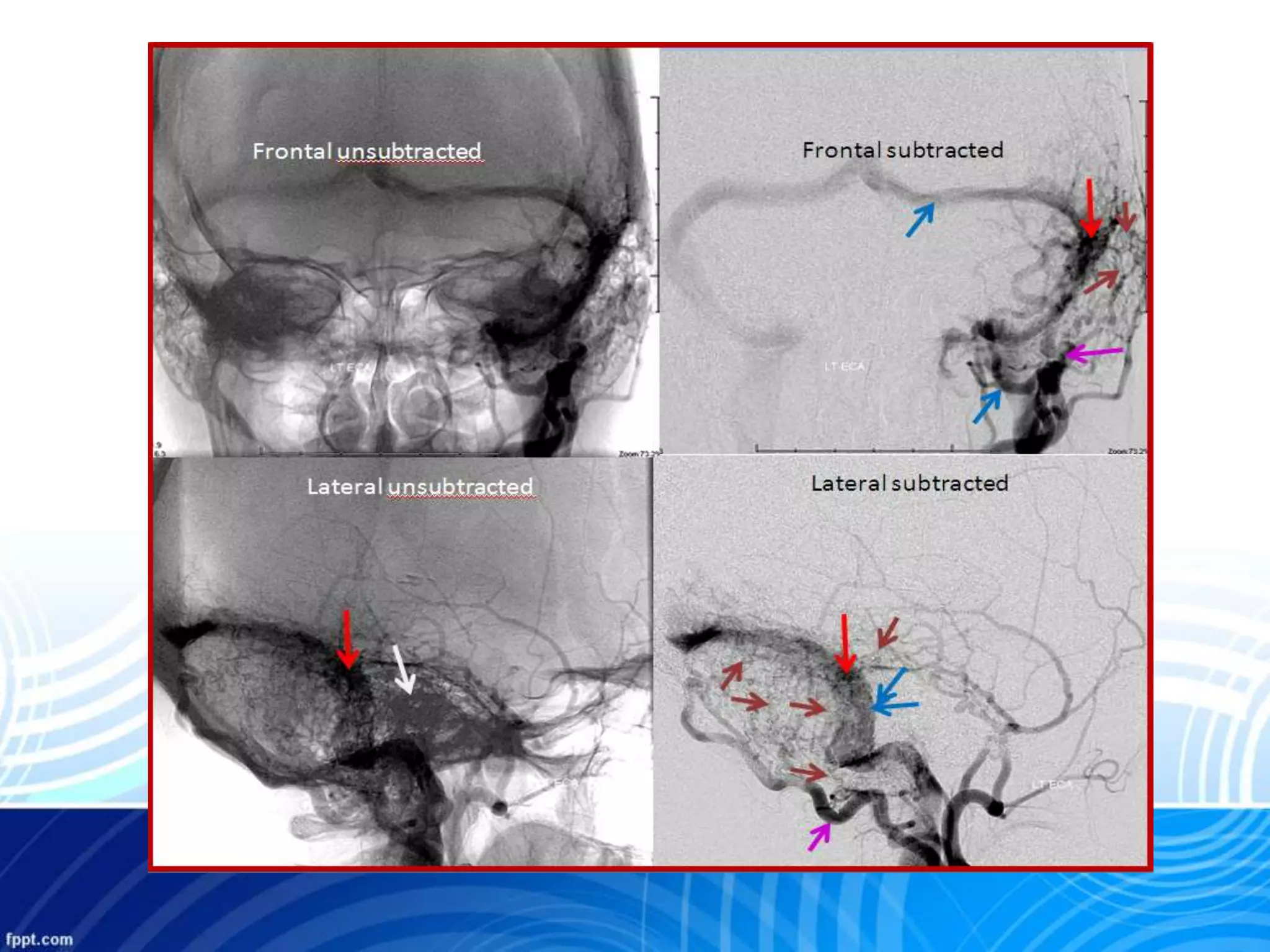
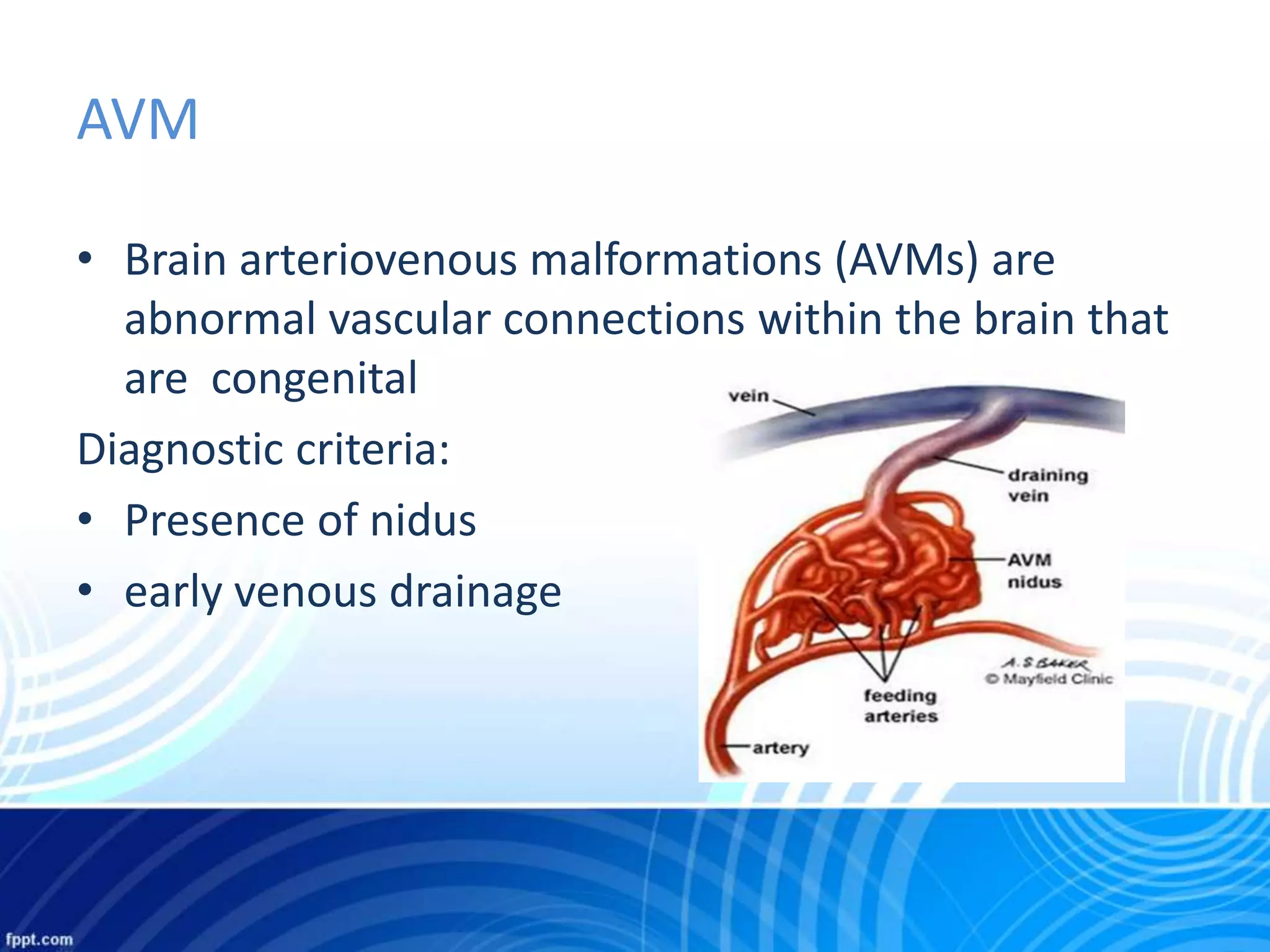
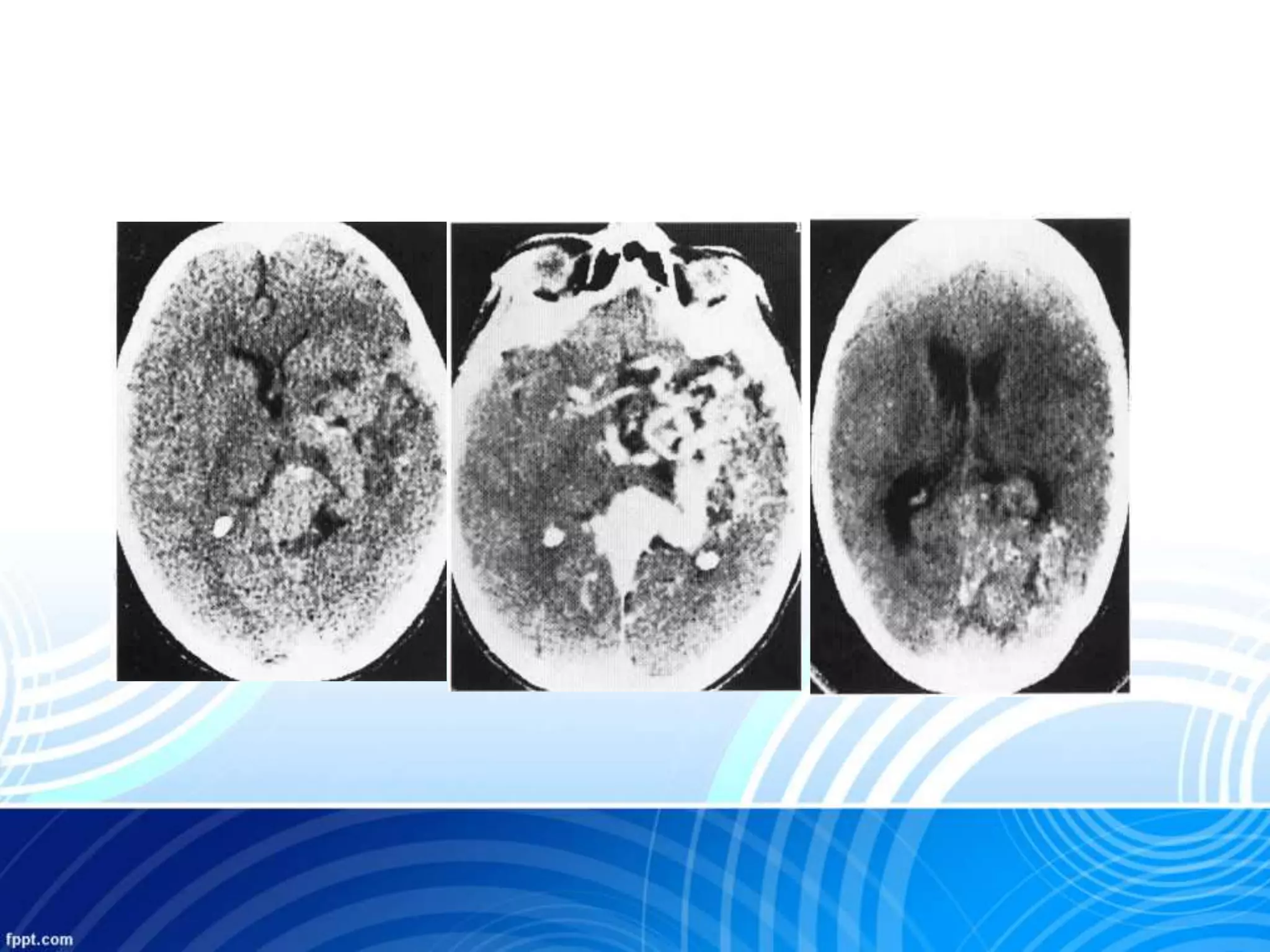
This document discusses various types of vascular malformations of the brain. It describes arteriovenous malformations (AVMs), dural arteriovenous fistulas (DAVFs), developmental venous anomalies (DVAs), cavernous malformations, and capillary telangiectasias. It provides details on imaging with angiography, CT, and MRI to identify these conditions. It also discusses treatments and classifications like the Borden system for DAVFs. Common locations are the transverse/sigmoid sinus for DAVFs and presentation can include pulsatile tinnitus, cranial nerve palsies, and hemorrhage.