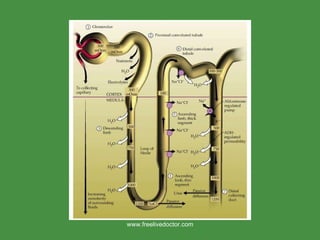
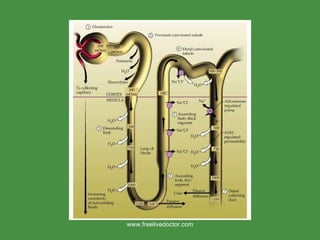
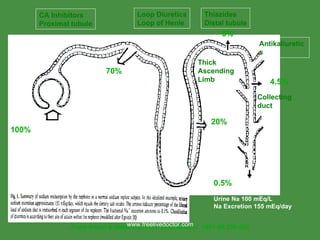
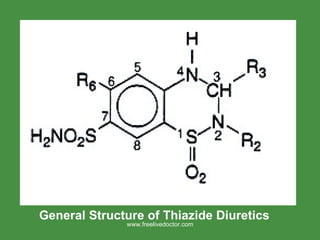
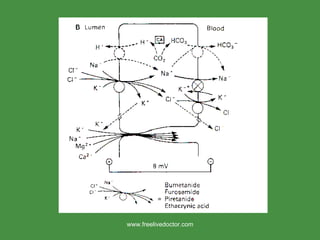
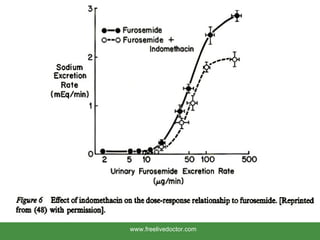
The document discusses drugs and their effects on the kidney. It covers normal kidney function, methods of assessing renal function, how drugs are processed by the kidneys, diuretics, nephrotoxic drugs, and prescribing considerations for patients with kidney disease. Key points include how different drug classes like loop diuretics and thiazides work at different sites in the nephron to cause diuresis, risks of nephrotoxicity from NSAIDs, aminoglycosides and contrast agents, and dosing adjustments needed in renal impairment.