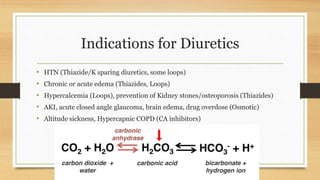
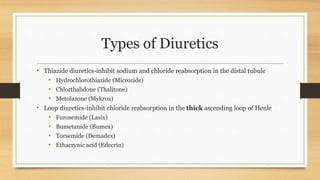
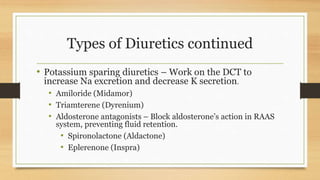
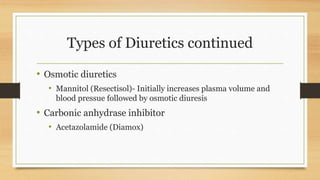
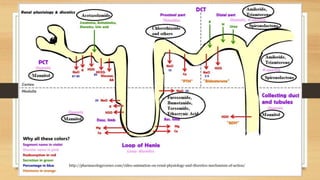
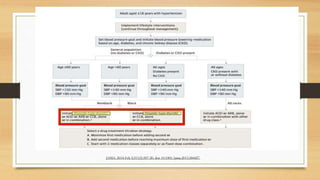
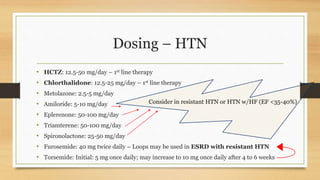
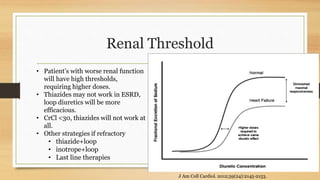
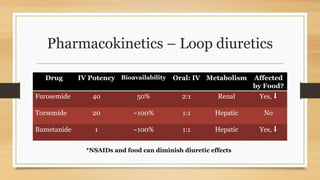
This document discusses diuretics, including their pharmacology, indications, types, dosing, and adverse effects. It covers the main classes of diuretics - thiazides, loop diuretics, potassium-sparing diuretics, osmotic diuretics, and carbonic anhydrase inhibitors. Key points include thiazide diuretics being first-line for hypertension, loop diuretics being used for more severe edema, and factors like renal function and food affecting diuretic dosing and efficacy. Adverse effects include electrolyte disturbances, hypotension, and renal impairment.