



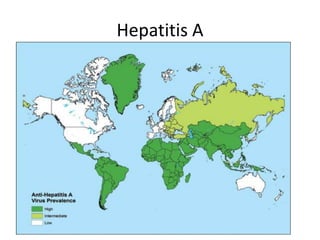
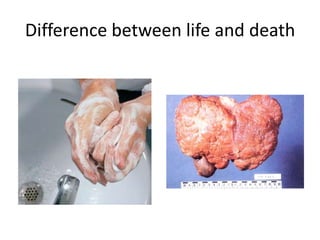

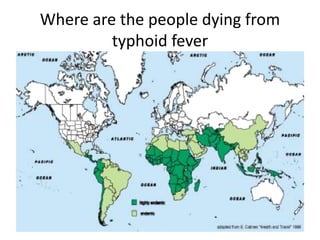






Hepatitis A and typhoid fever are vaccine-preventable waterborne diseases transmitted through the fecal-oral route. They remain a major public health issue in Pakistan, with over two-thirds of the population lacking access to clean drinking water. Typhoid fever in particular is endemic in Pakistan, with high rates of multidrug-resistant Salmonella strains emerging. Vaccination is critical to control these diseases and reduce their significant health and economic burden.











































































































