Downloaded 26 times





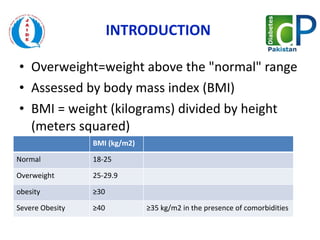
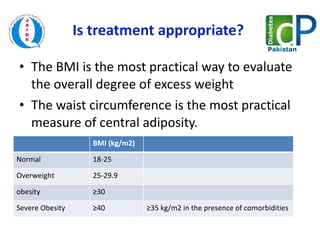



This document discusses the management of obesity through various treatment options. It defines obesity as a BMI of 30 or higher. Treatment options discussed include behavioral modification through diet and exercise, pharmacological therapies, liposuction, and bariatric surgery for severe obesity. The most appropriate treatment depends on a patient's BMI and any comorbidities, with lifestyle changes and drugs recommended before considering surgery.



































































































