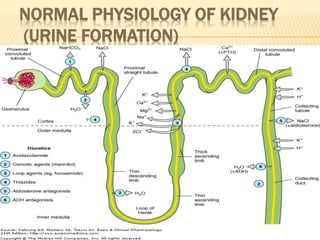
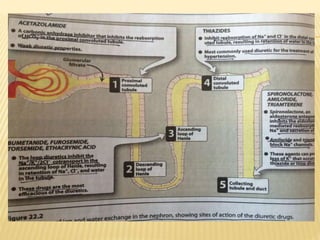
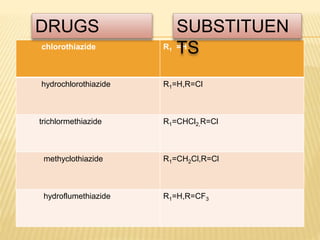
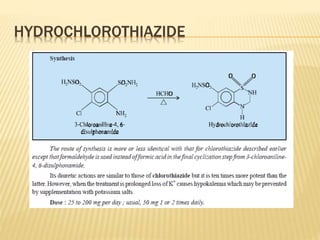
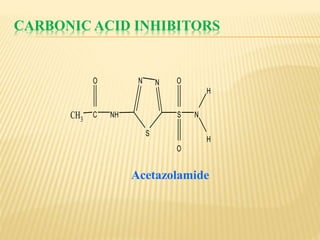
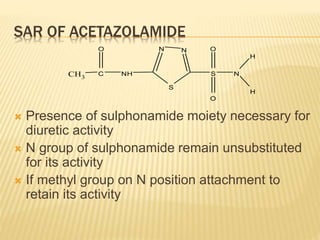
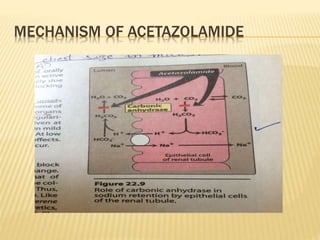
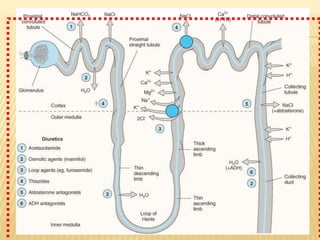
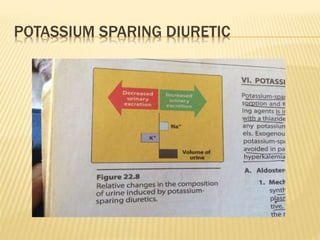
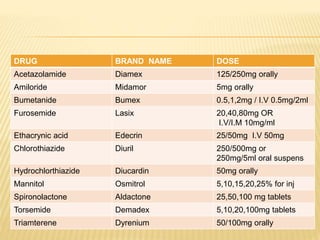
Diuretics are drugs that increase urine output by inhibiting reabsorption of sodium, chloride and water in the kidneys. There are several classes of diuretics including thiazide diuretics, loop diuretics, carbonic anhydrase inhibitors, and potassium-sparing diuretics. Thiazide diuretics such as chlorothiazide and hydrochlorothiazide act by inhibiting sodium reabsorption in the distal convoluted tubule. Loop diuretics like furosemide act in the loop of Henle and are the most potent class. Carbonic anhydrase inhibitors including acetazolamide inhibit bicarbonate reabsorption in the proximal tubule. Potassium-spar