Acute Shoulder dislocation is an orthopaedic emergency where the humeral head is displaced from the glenoid fossa. There are different types of shoulder dislocations including anterior, posterior, inferior and superior. Anterior dislocations are the most common, comprising around 90% of cases. Clinical presentations vary depending on the type of dislocation but may include pain, swelling, bruising, weakness and restricted range of motion. X-rays can confirm the diagnosis and type of dislocation. Several techniques can be used to reduce the shoulder joint, the most common being the Kocher method for anterior dislocations and traction-countertraction for posterior dislocations.
Overview of shoulder dislocation as a common orthopedic emergency, affecting mainly males aged 21-30 and females 61-80.
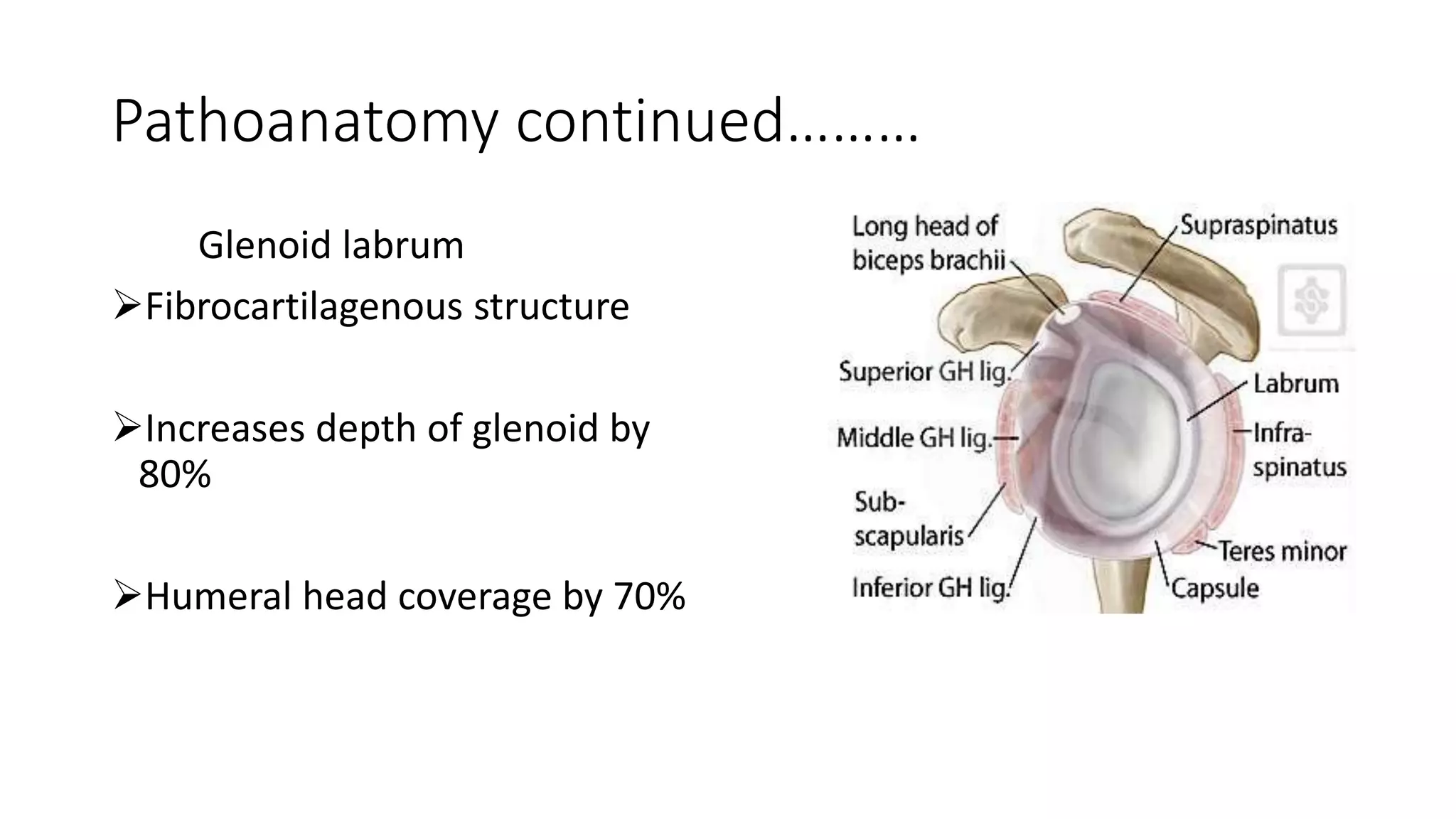
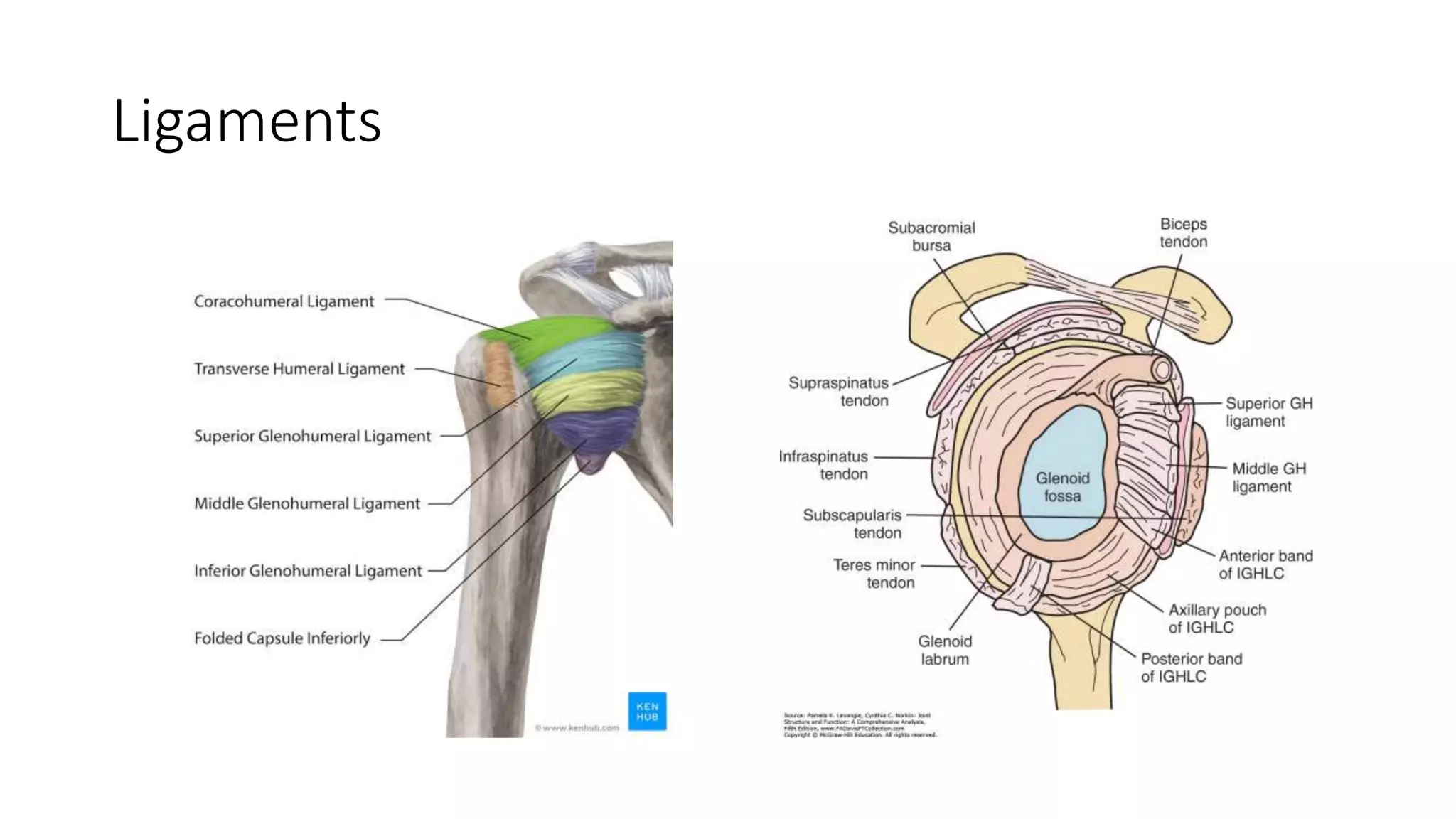
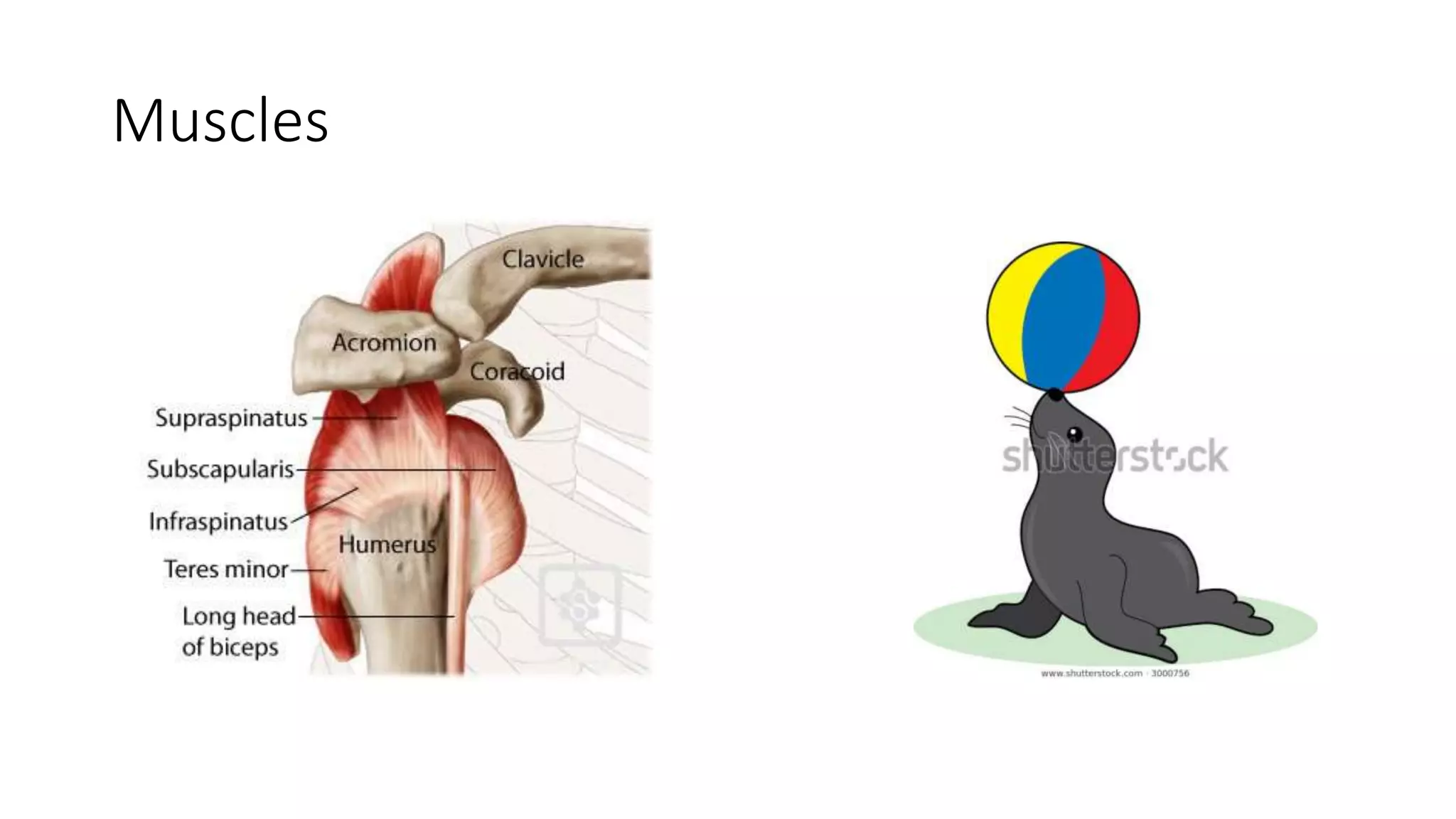
Description of the shoulder's anatomy including its ligaments, joint capsule, muscles, and their role in stability and movement.
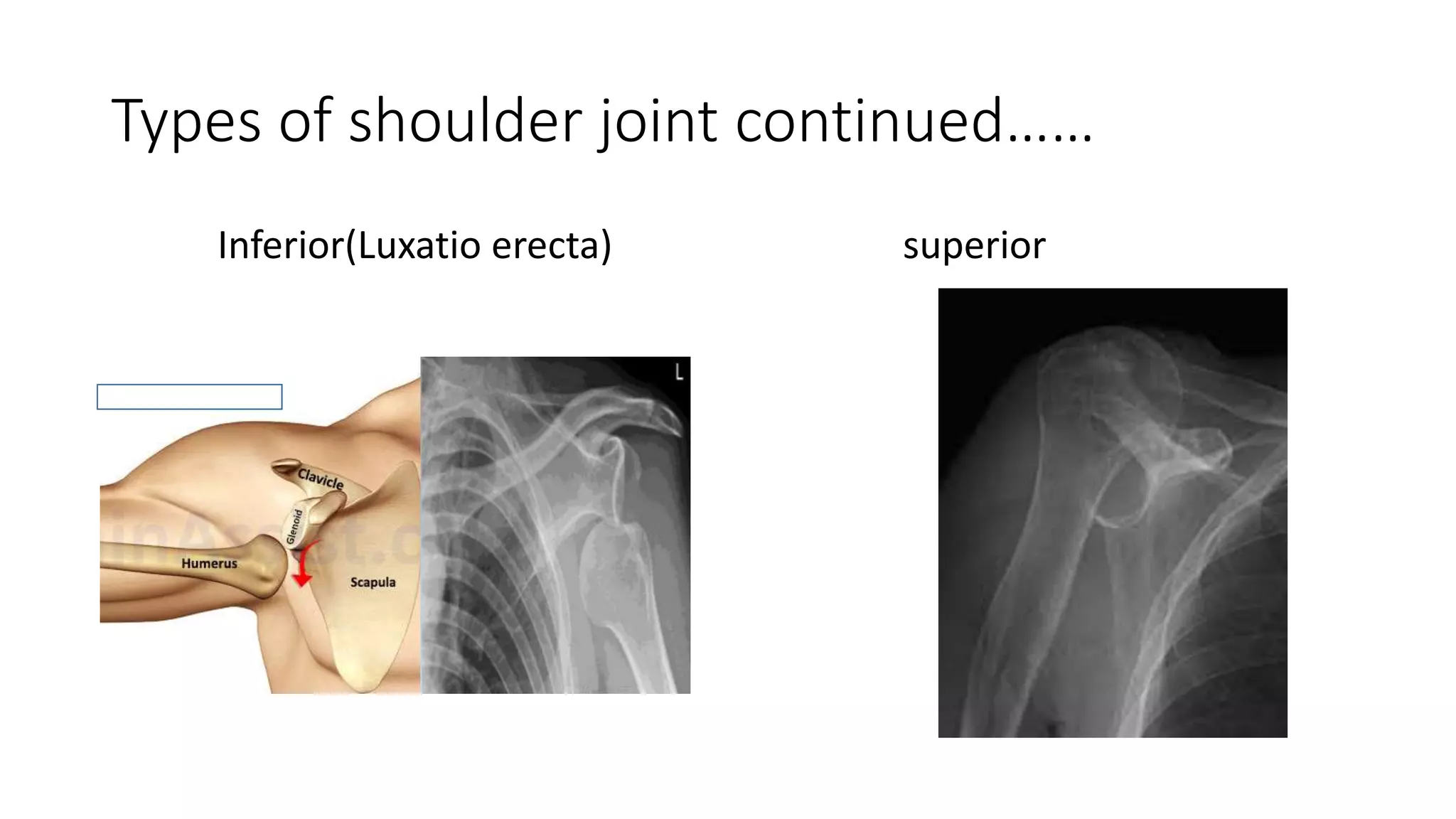
Classification of shoulder dislocations, noting that anterior dislocations account for 90%.
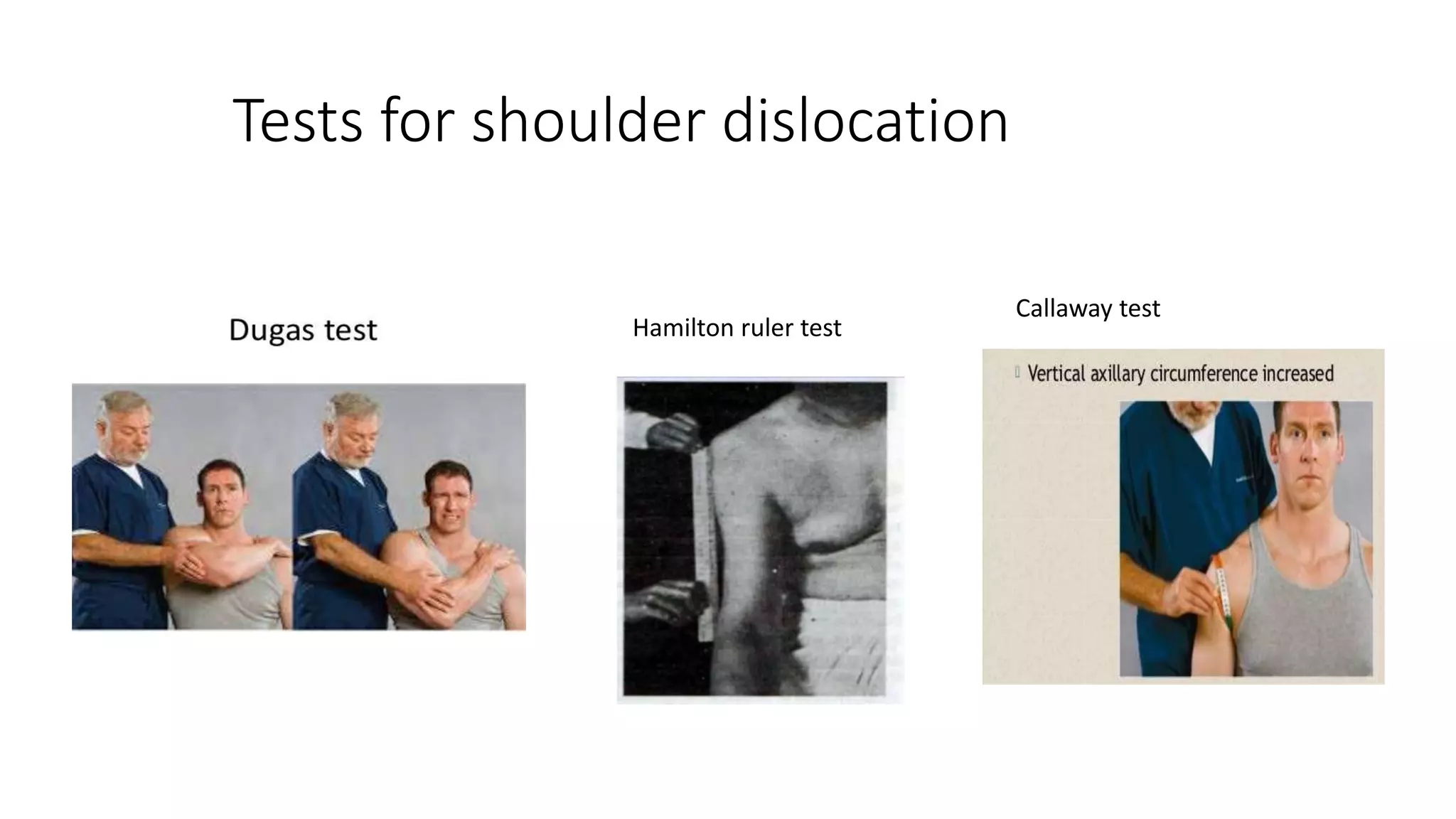
Symptoms and signs related to dislocations, including trauma history and physical findings.
Utilization of various tests and imaging techniques such as X-rays, ultrasound, and CT for dislocation detection.
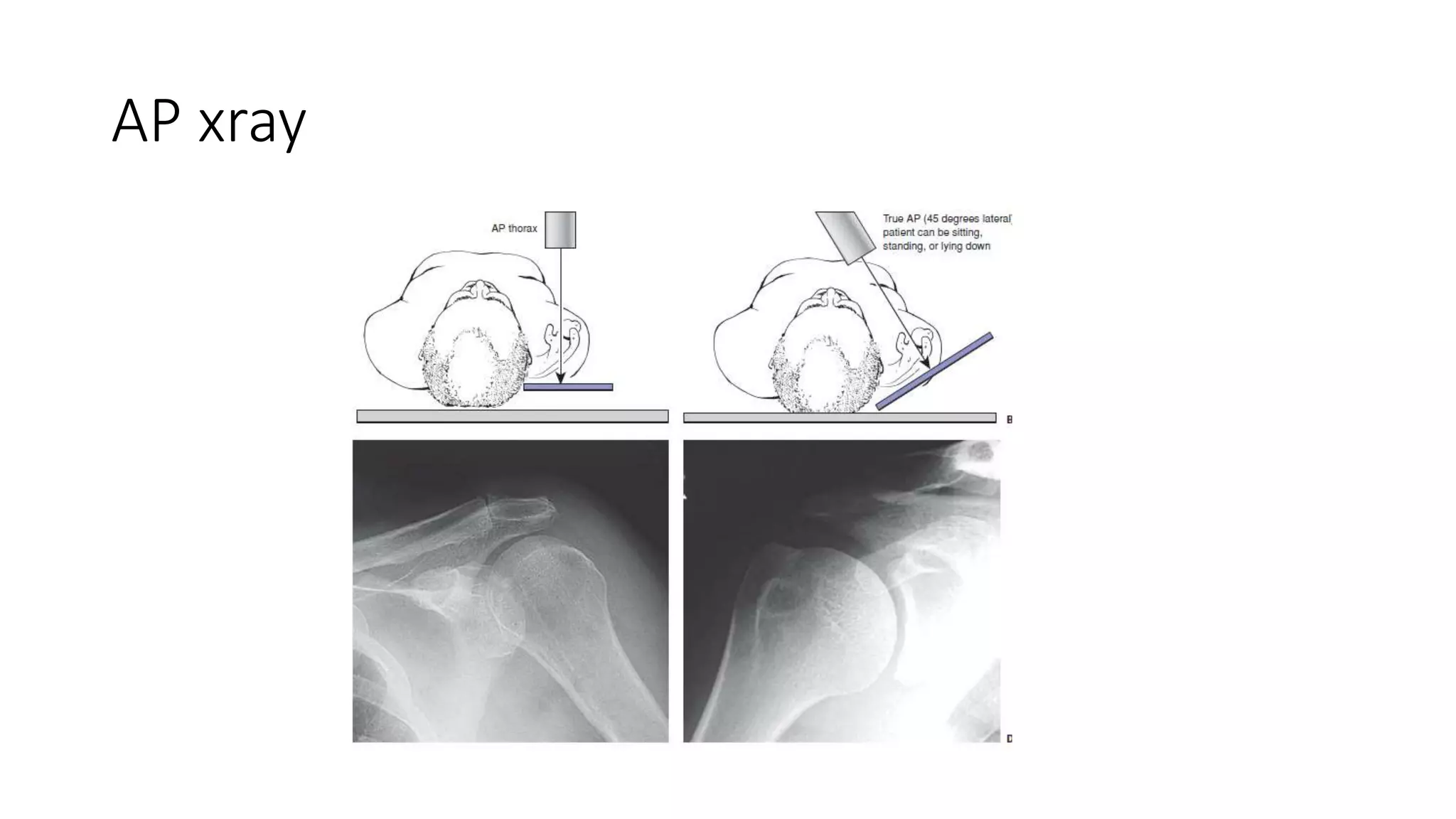
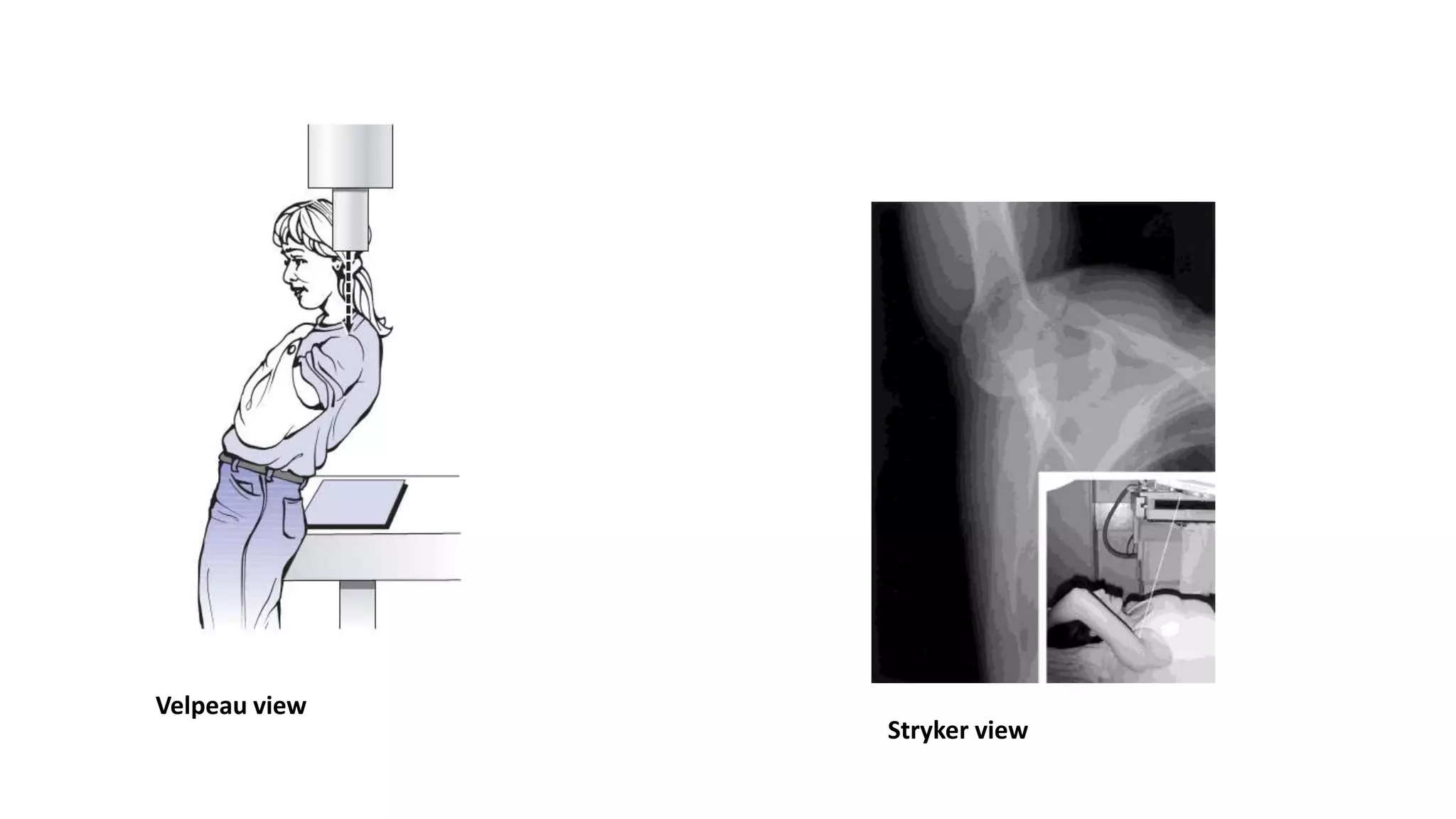
Specific X-ray views used to diagnose shoulder dislocations, including the AP chest and specialized views.
Overview of various reduction techniques for shoulder dislocations, including Kocher’s and Hippocratic methods.Citations of resources used for the presentation and a thank you note.
Introduction
• Dislocations areothopaedic emergencies
• Shoulder dislocation comprises of up to half of all joint dislocations
• Most mobile and most commonly dislocated joint of body
• Incidence: Male:21-30yrs Female:61-80yrs
Function of shoulder
Movementstability
Ball and socket
joint
Voluminous glenohumeral
joint
Ligaments at extremes
of motions
muscles
Unstable joint
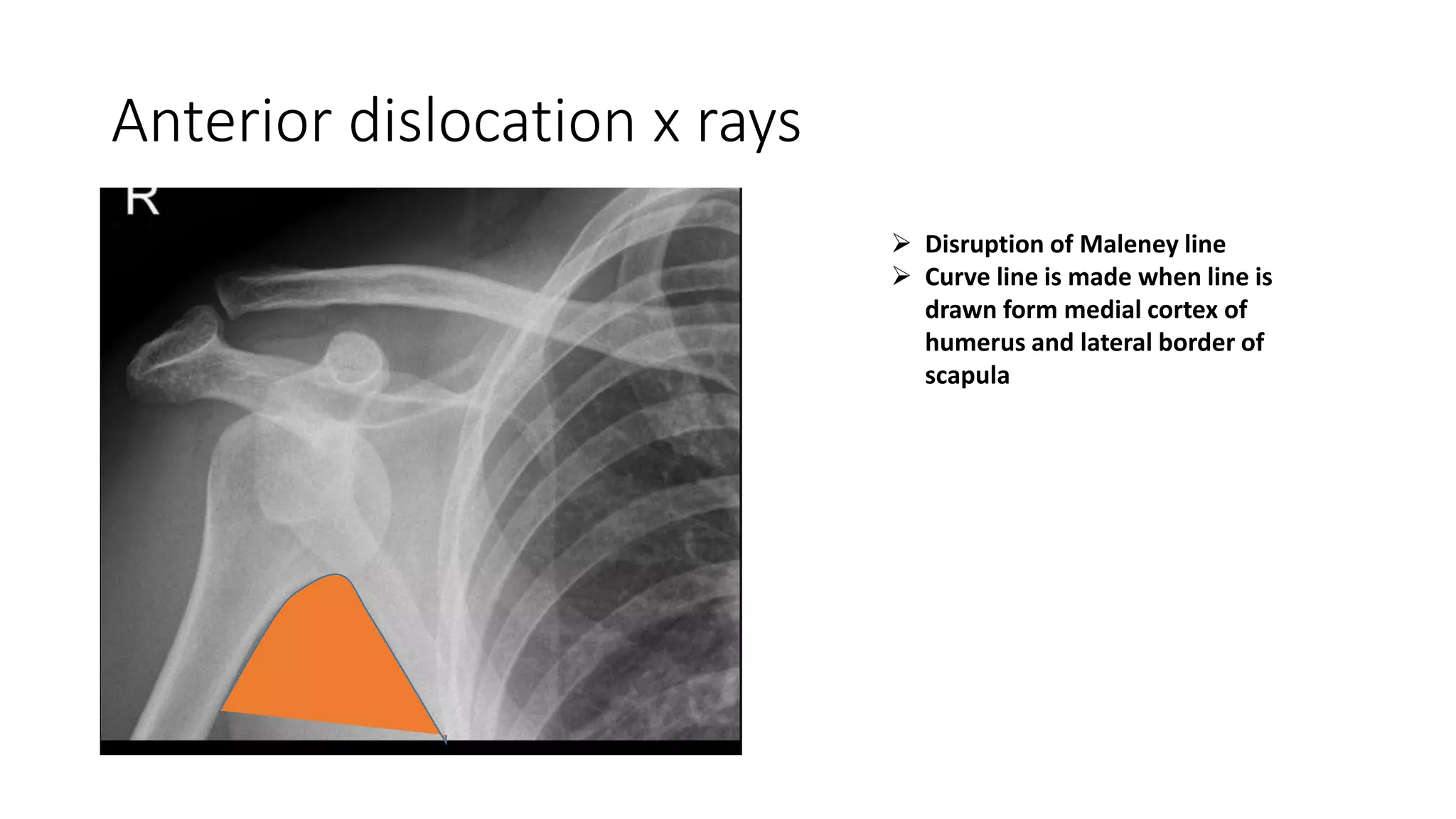
Anterior dislocation xrays
Disruption of Maleney line
Curve line is made when line is
drawn form medial cortex of
humerus and lateral border of
scapula
22.
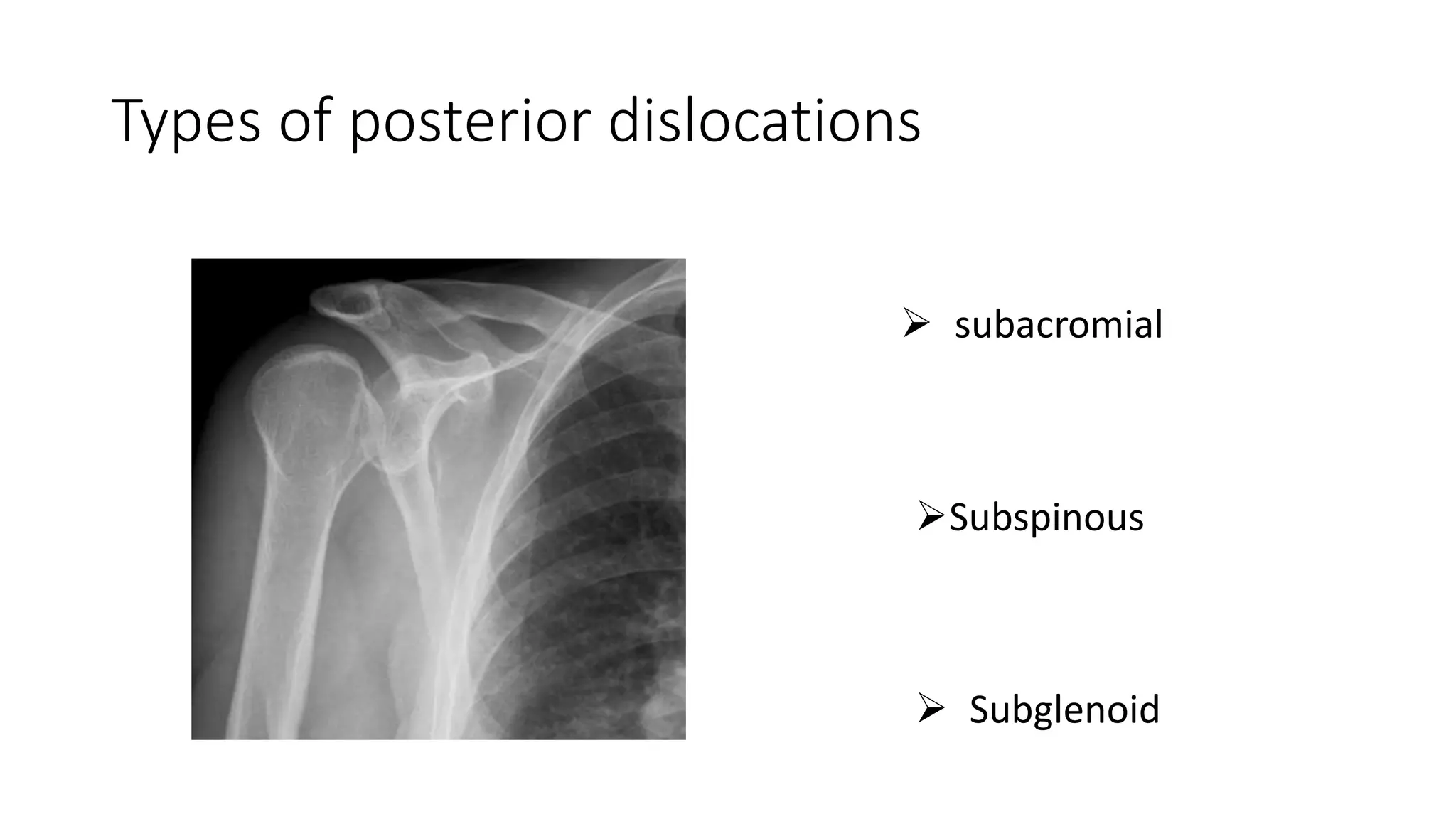
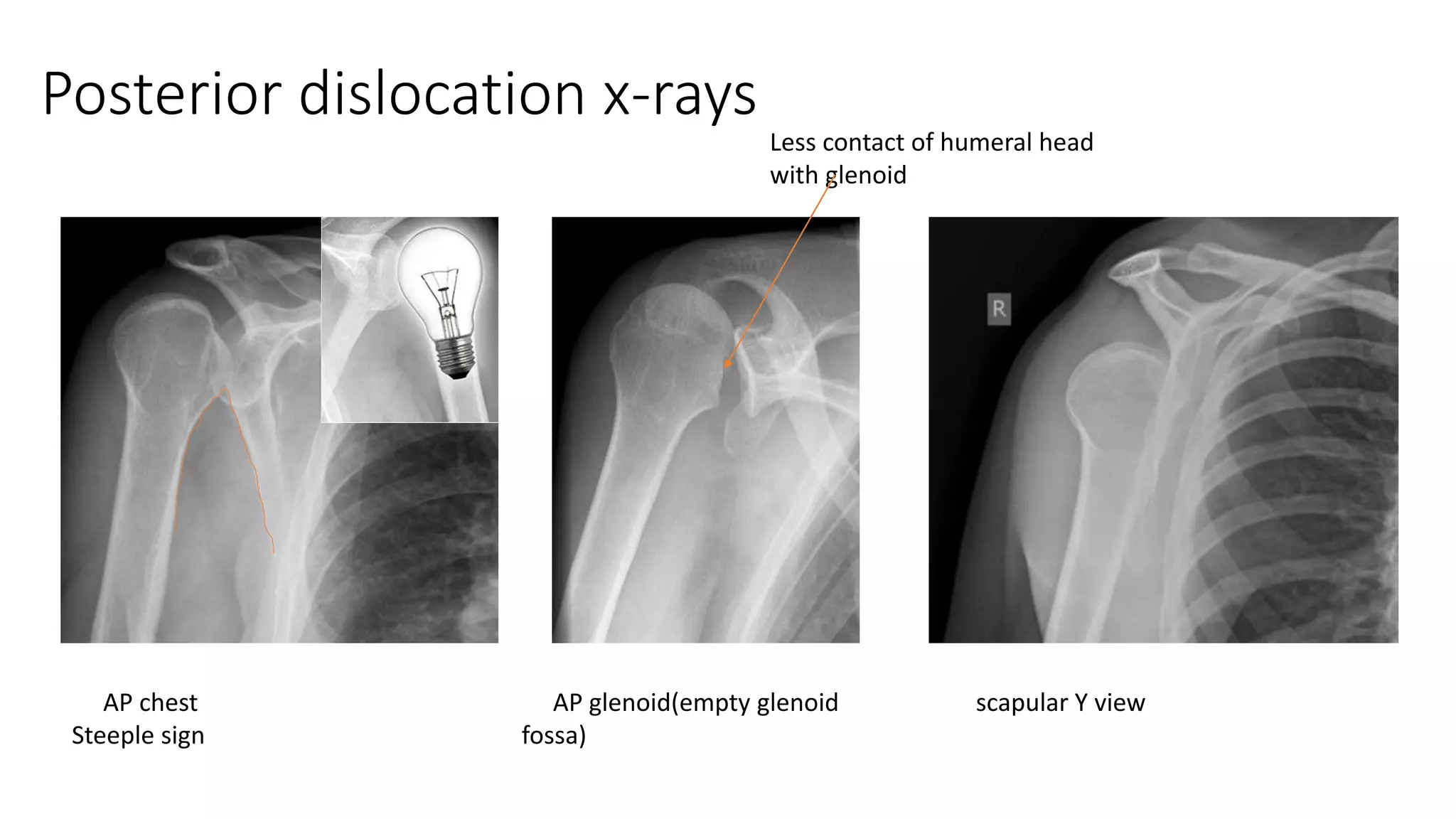
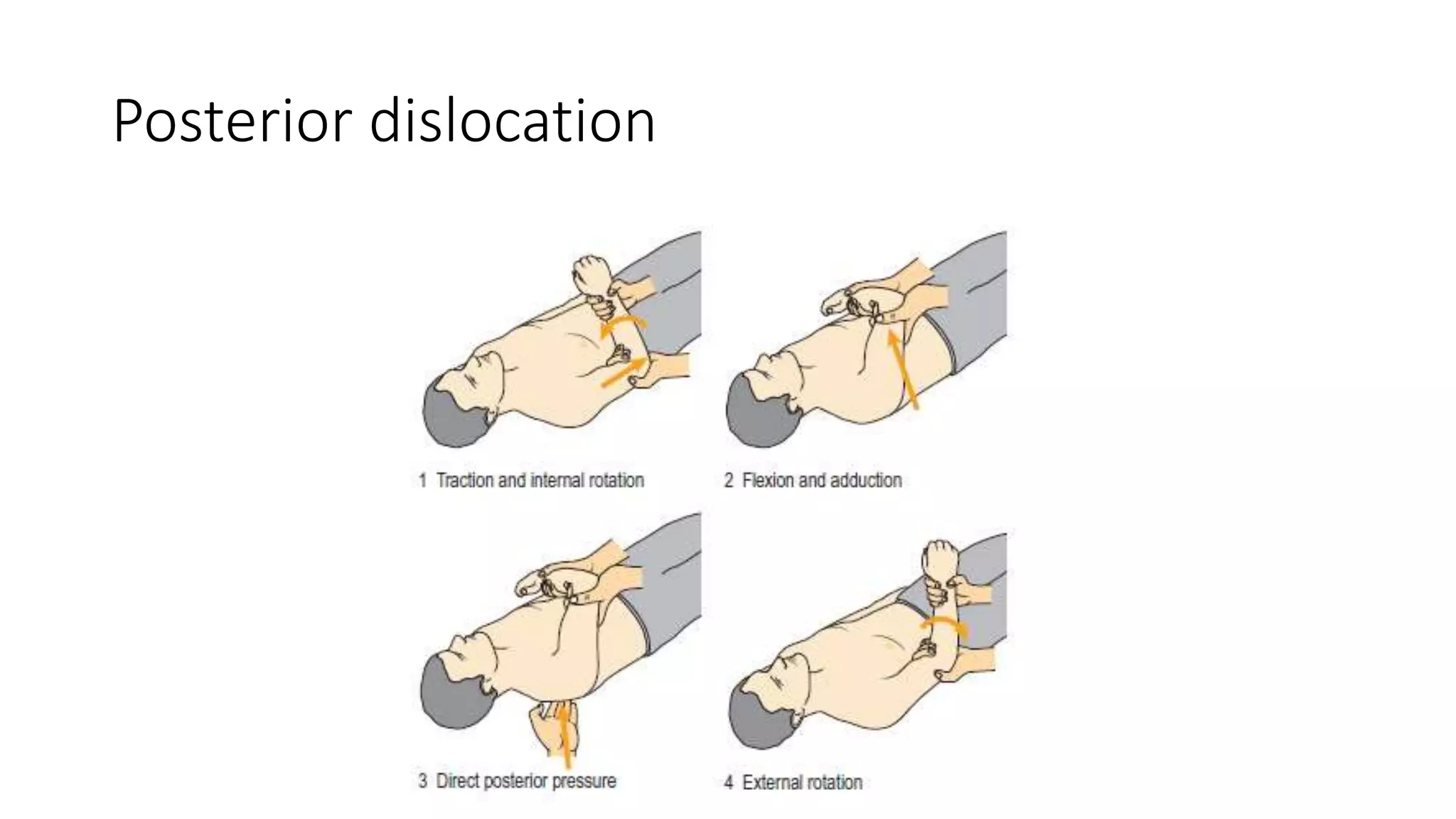
Posterior dislocation x-rays
APchest
Steeple sign
AP glenoid(empty glenoid
fossa)
scapular Y view
Less contact of humeral head
with glenoid
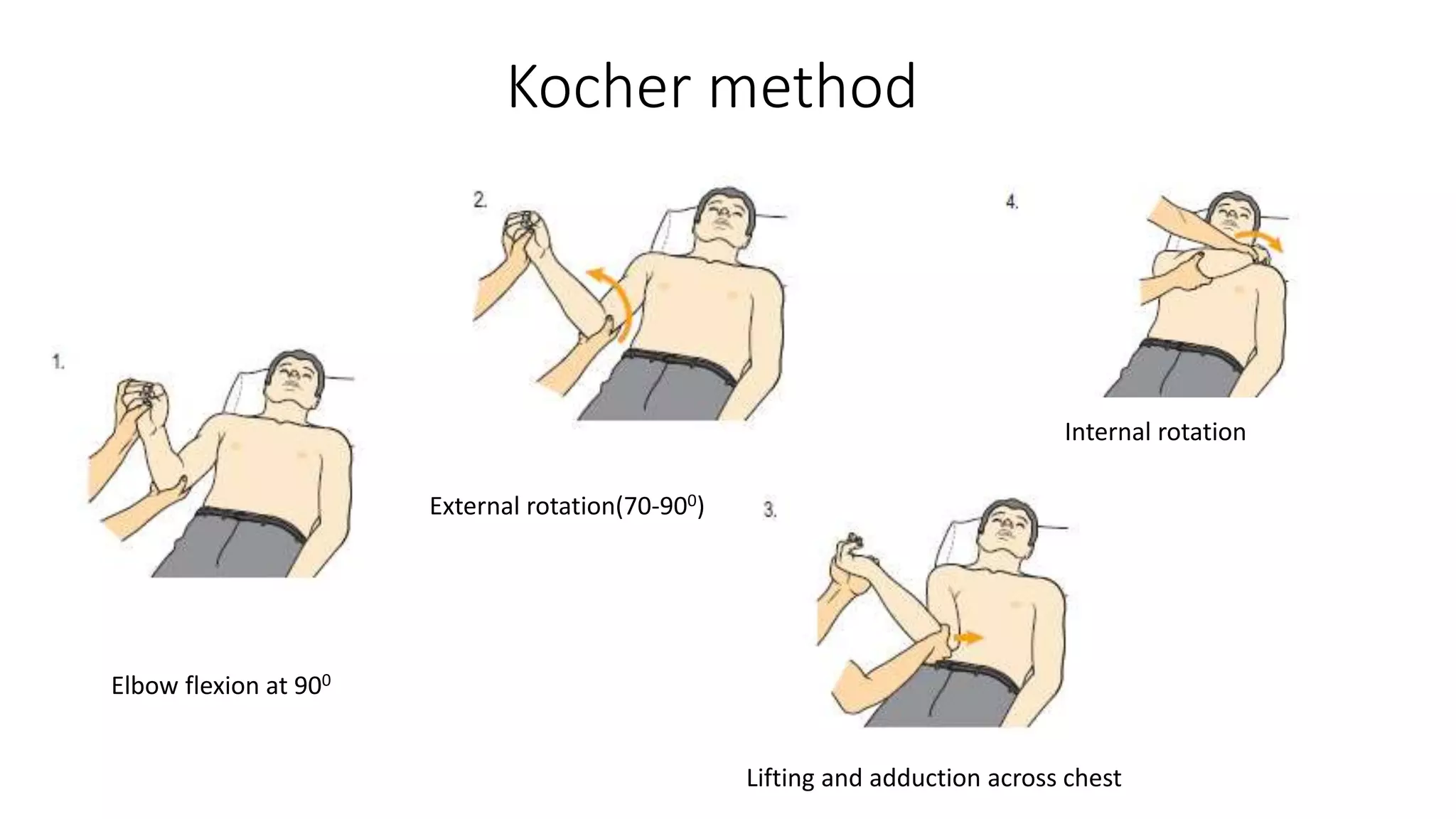
Kocher method
Elbow flexionat 900
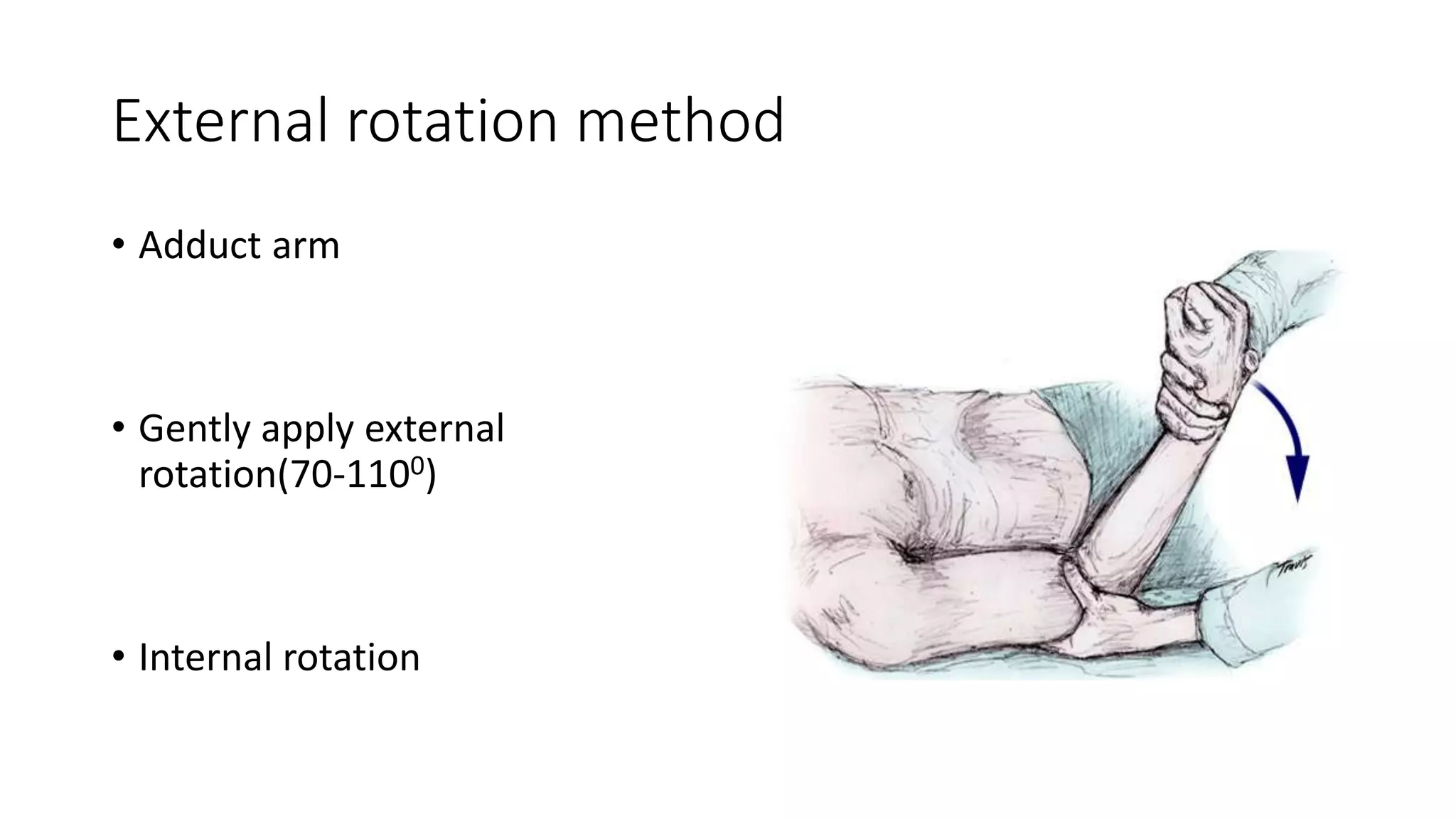
External rotation(70-900)
Lifting and adduction across chest
Internal rotation
25.
Hippocratic method
• Patientis placed supine
• Stockinged heel is placed in the
axilla
• Wrist is grasped in both hand
and gentle traction and external
rotation is given
• Heel acts as fulcrum while
adduction arm
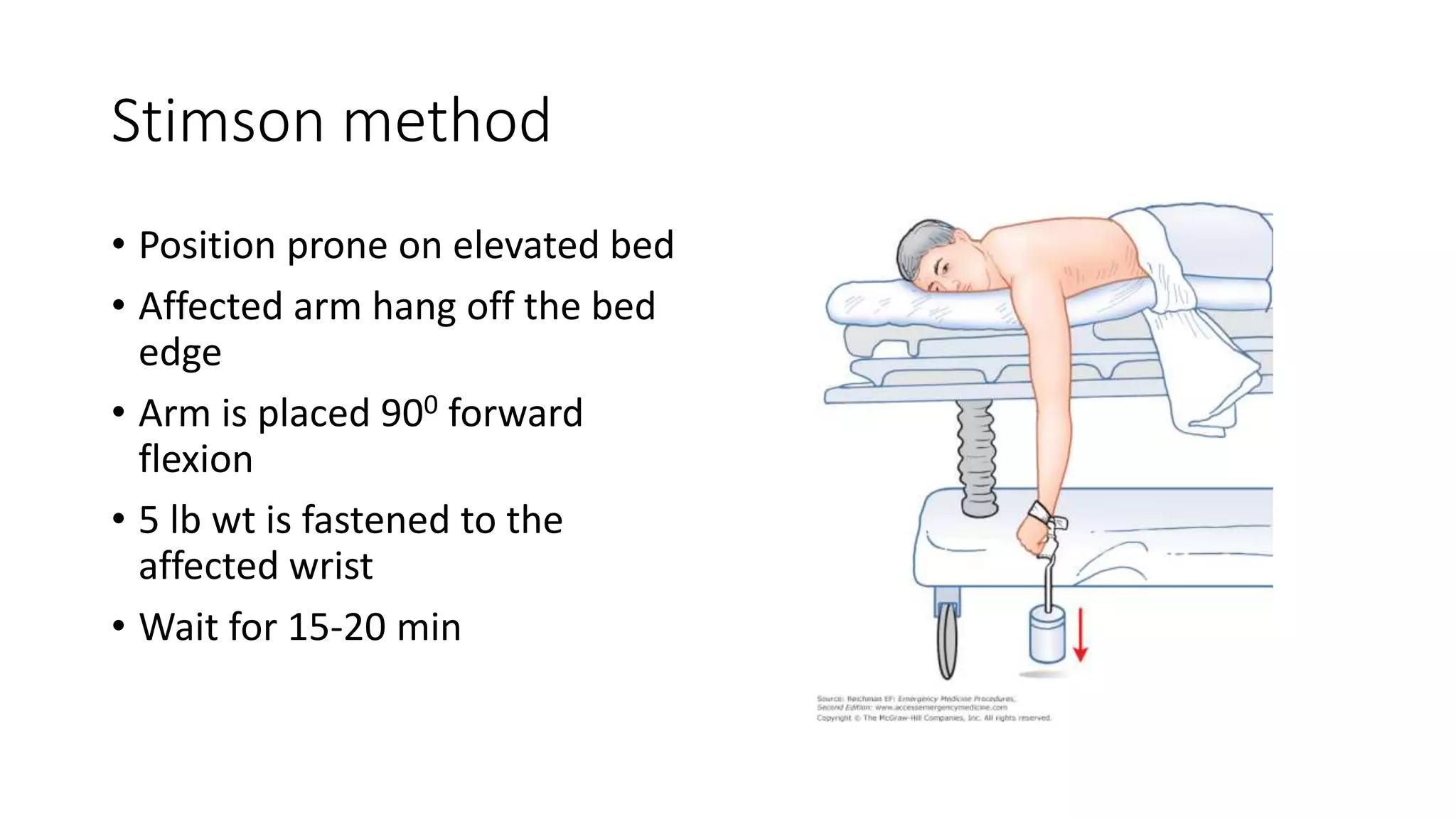
Stimson method
• Positionprone on elevated bed
• Affected arm hang off the bed
edge
• Arm is placed 900 forward
flexion
• 5 lb wt is fastened to the
affected wrist
• Wait for 15-20 min
28.
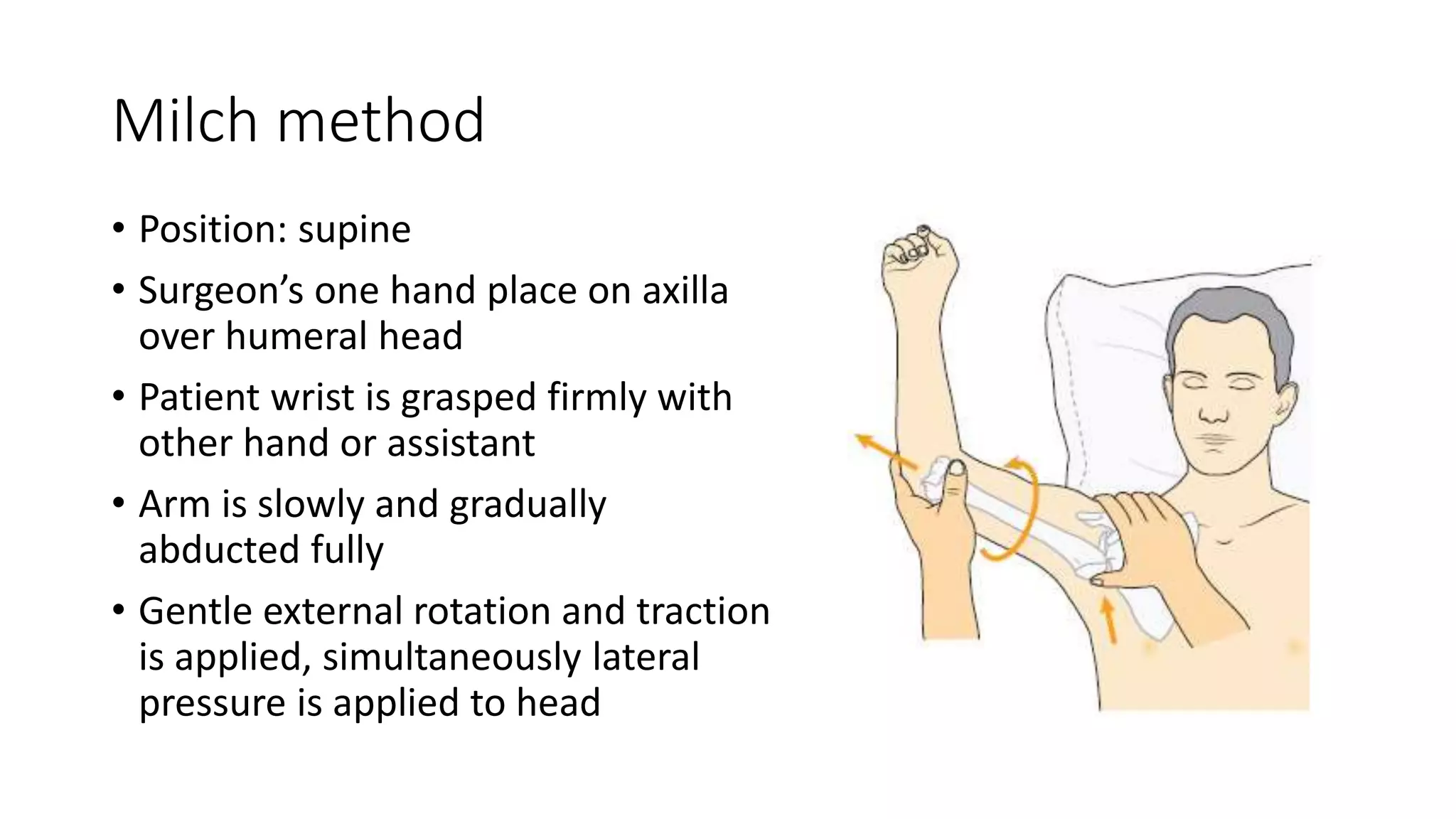
Milch method
• Position:supine
• Surgeon’s one hand place on axilla
over humeral head
• Patient wrist is grasped firmly with
other hand or assistant
• Arm is slowly and gradually
abducted fully
• Gentle external rotation and traction
is applied, simultaneously lateral
pressure is applied to head
29.
Spaso Method
• Withpatient supine on bed,
physician grasps the affected
distal forearm
• Lift arm vertically to ceiling
applying gentle traction and
external rotation
• Audible clunk is heard, if not
give direct pressure to humeral
head
30.
Scapular manipulation
• Scaupulais manipulated using
physician’s hand
• Inferior tip is rotated medially and
displaced superiorly













![References
• McRae’s Orthopaedic Trauma and Emergency Fracture management
3rd edition
• Rockwood and Greens Fractures in Adults - 2 Volume Set [8th
ed][2014][
• Apley’s system of orthopaedics and fractures, 10th edition
• Campbell’s operative otrhopaedic, 13edition
• Mescape, reduction of shoulder dislocation](https://image.slidesharecdn.com/acuteshoulderdislocation-200213124049/75/Acute-shoulder-dislocation-34-2048.jpg)




































































