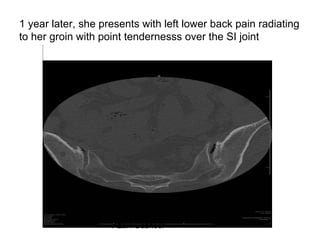
Downloaded 190 times




![Summary
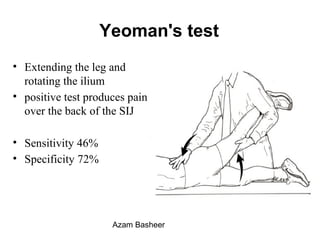
Positive provocative maneuvers combined with 75% pain
relief after image guided SI joint injection is a reliable
method for diagnosing the SI joint as the pain generator
A positive response to low-volume anesthetic injection into
the sacroiliac joint is required before considering
surgery.
Patients should have failed at least 6 months of
conservative treatment (physical therapy, nonsteroidal
anti-inflammatory drugs [NSAIDs], exercise, and
therapeutic injections) before considering surgical fusion
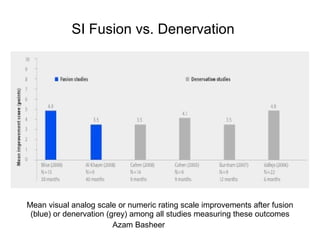
The open fusion studies reported poorer results and higher
complication rates than the percutaneous studies.
Azam Basheer](https://image.slidesharecdn.com/b3f7b43b-7cbd-4631-a627-cb95330fc14c-150401222933-conversion-gate01/85/SI-joint-Fusion-Azam-Basheer-MD-61-320.jpg)

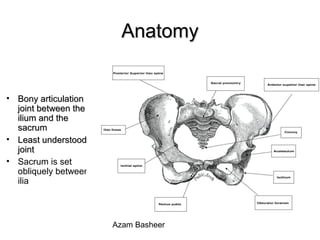
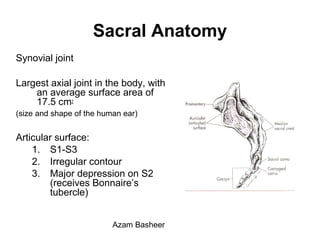
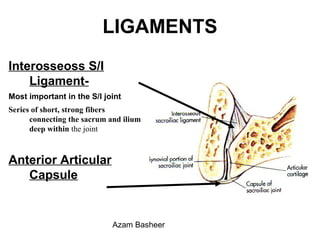
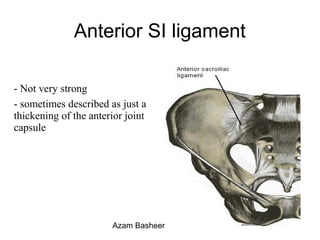
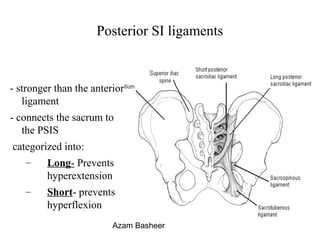
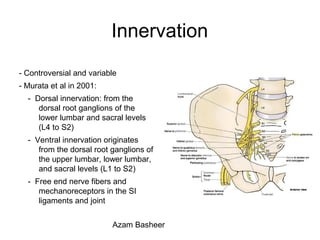
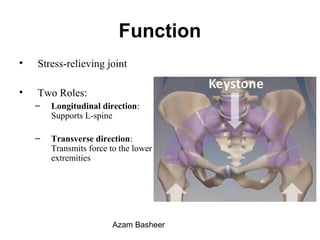
The document discusses the sacroiliac joint (SIJ), including its anatomy, biomechanics, evaluation, and treatment options for SIJ pain. Key points include: - The SIJ is a synovial joint between the sacrum and ilium bones that allows limited motion. It is innervated by lumbar and sacral nerve roots and plays a role in stress relief and force transmission. - Evaluation of SIJ pain is challenging due to its anatomy. History, physical exam maneuvers like Patrick's test, and image-guided injections are used to diagnose SIJ pain. - Treatment options for SIJ pain include conservative care, injections, denervation, and fusion surgery. Per
















































































![POUR AANS 1226 presentation A. Bashee[1]](https://cdn.slidesharecdn.com/ss_thumbnails/43b146c4-09cd-4359-a214-100e086d503d-150401212237-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)