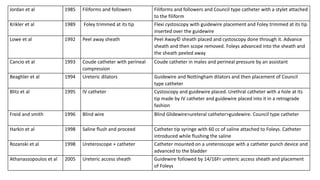
The document discusses tips for successful urethral catheterization, including pre-treating the urethra with lubricant or anesthetic gel, positioning the patient properly, and using different catheter sizes and techniques if initial attempts fail. It also covers evaluating and managing specific causes of difficult catheterization like phimosis, edema, spasm, and various obstructions. The document provides an algorithm and references for managing difficult urethral catheterization cases.