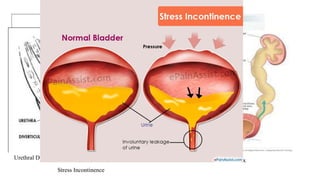
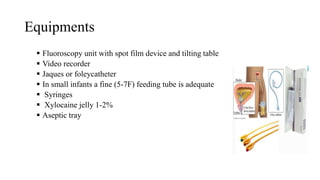
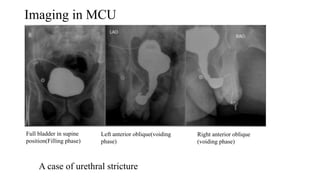
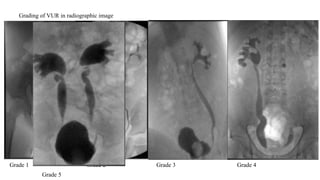
MCUG is a radiographic procedure used to evaluate the urinary tract. Contrast medium is injected into the bladder under fluoroscopy and images are taken as the patient voids to check for any reflux of contrast into the ureters or kidneys. It is used to investigate conditions like urinary tract infections, vesicoureteral reflux, and incontinence. The procedure involves catheterizing the bladder, filling it with contrast, and taking spot images during voiding to check for reflux. Precautions like using low-dose techniques are important to reduce radiation exposure, especially in pediatric patients.