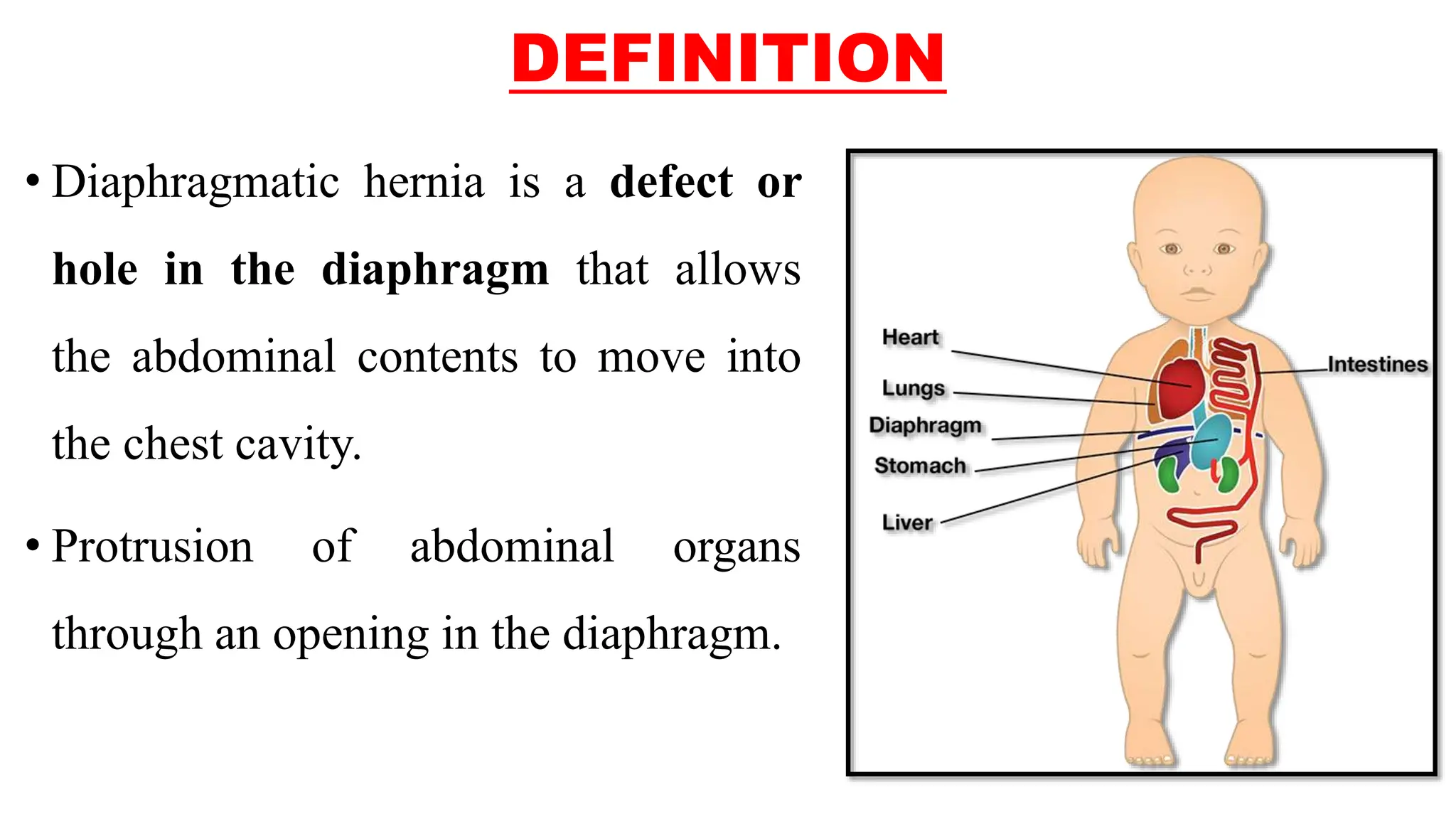
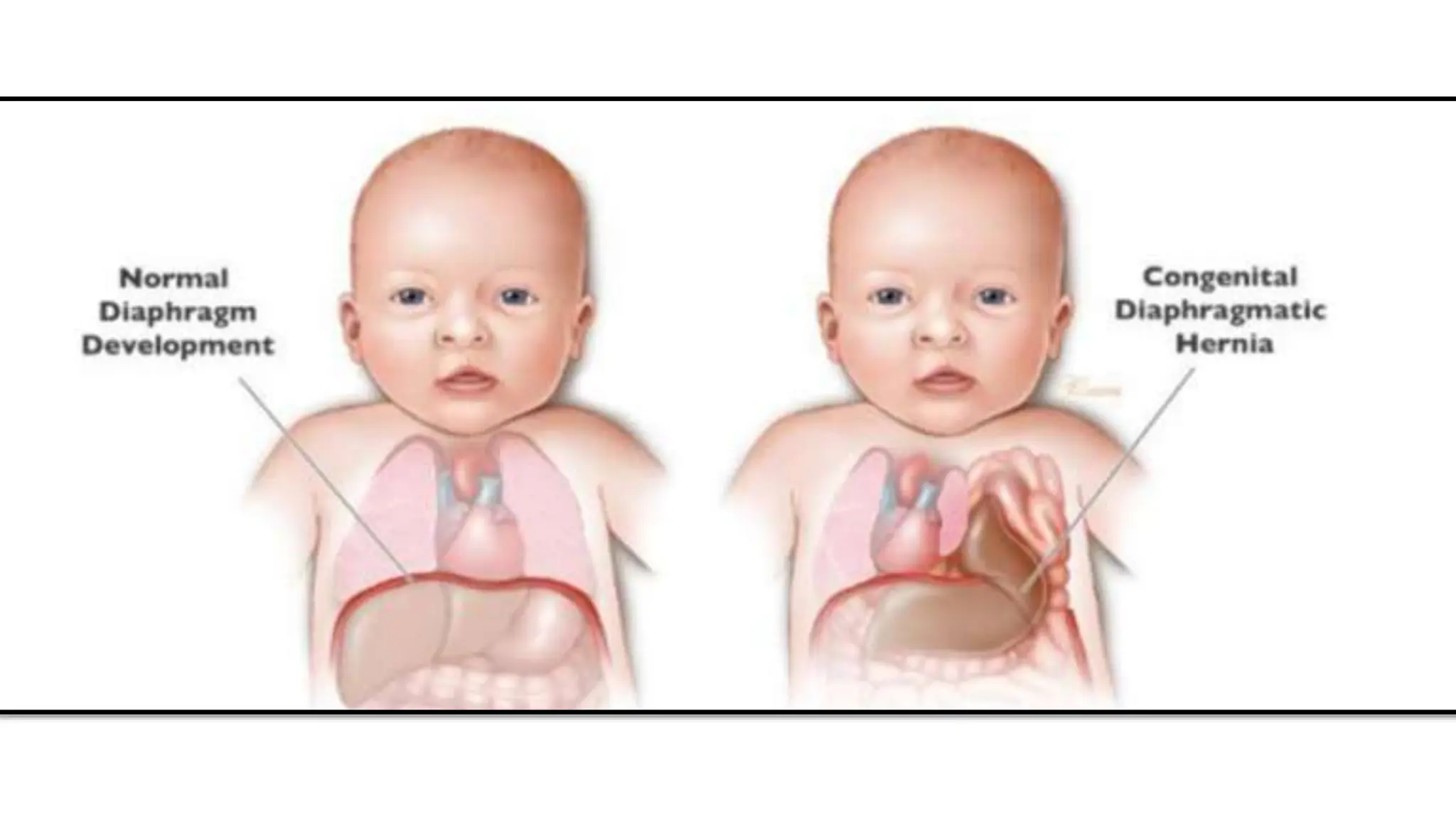
Congenital diaphragmatic hernia (CDH) is a defect in the diaphragm that allows abdominal contents to enter the chest cavity, impacting lung development and occurring in 1 in 2,500-4,000 births. The two types are Bochdalek hernia, more common on the left side, and Morgagni hernia, which is rare and occurs in the middle of the diaphragm. Diagnosis often happens via prenatal ultrasound, and treatment may include ECMO, surgical repair, and additional medical interventions depending on severity.




















































![CONGENITAL DIAPHRAGMATIC HERNIA [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congenitaldiaphragmaticherniarecovered-240421180720-5c4f960f-thumbnail.jpg?width=640&height=640&fit=bounds)






















































