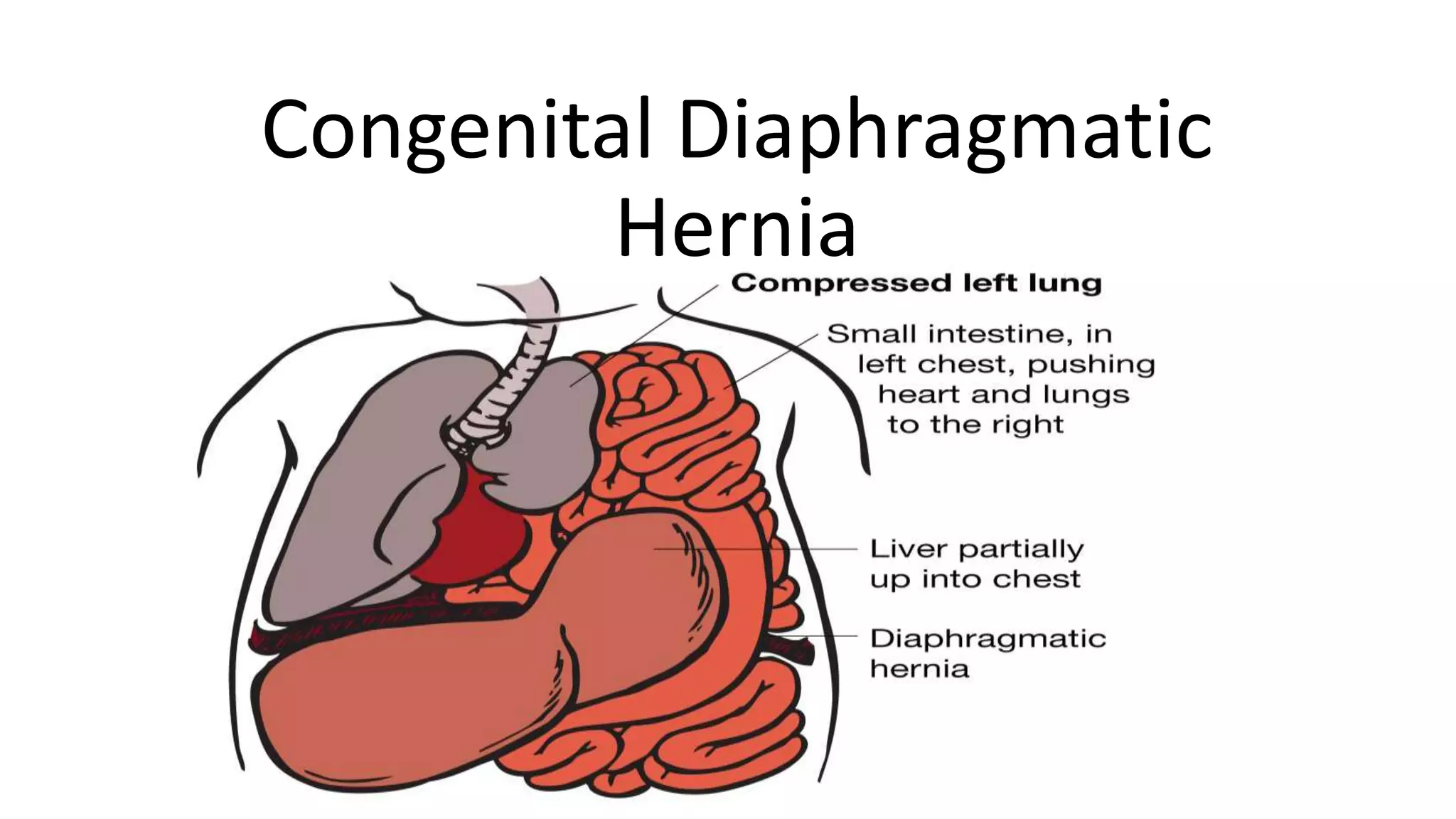
Congenital diaphragmatic hernia (CDH) is a birth defect where abdominal organs protrude into the chest cavity through an opening in the diaphragm. There are three main types - Bochdalek (most common), Morgagni, and hiatal hernias. CDH occurs when the diaphragm fails to fully develop, usually resulting from defects in the pleuroperitoneal membranes or diaphragmatic musculature. Prenatal ultrasound can detect over 70% of CDH cases. Postnatal management focuses on gentle ventilation strategies and optimizing the infant's condition before surgical repair of the diaphragmatic defect. Outcomes are best when care is provided at specialized


![ETIOLOGY
• CDH occurs when the muscular entities of the diaphragm fail to develop
normally, resulting in displacement of abdominal components into the
thorax.
• Bochdalek hernia
• Bochdalek hernias[6] make up the majority of cases of CDH. The major
problem in these hernias is posterolateral defects of the diaphragm, which
results in either failure in the development of the pleuroperitoneal folds or
improper or absent migration of the diaphragmatic musculature.
• As many as 90% of patients with CDH present in the neonatal period or
within the first year of life. These cases have a mortality of 45-50%. Most of
the morbidity and mortality of CDH relates to hypoplasia of the lung and
pulmonary hypertension on the affected side.](https://image.slidesharecdn.com/congenitaldiaphragmatichernia-210702182859/75/Congenital-diaphragmatic-hernia-6-2048.jpg)
![• Morgagni hernia
• Morgagni hernia [7, 8, 9] is a less common CDH, accounting for only 5-
10% of CDH cases. The foramen of a Morgagni hernia occurs in the
anterior midline through the sternocostal hiatus of the diaphragm,
with 90% of cases occurring on the right side.](https://image.slidesharecdn.com/congenitaldiaphragmatichernia-210702182859/75/Congenital-diaphragmatic-hernia-7-2048.jpg)





















![CONGENITAL DIAPHRAGMATIC HERNIA [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congenitaldiaphragmaticherniarecovered-240421180720-5c4f960f-thumbnail.jpg?width=640&height=640&fit=bounds)





























































