Downloaded 212 times

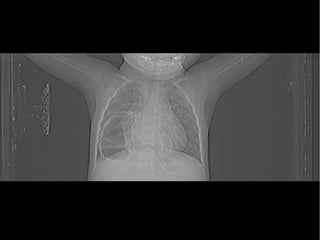
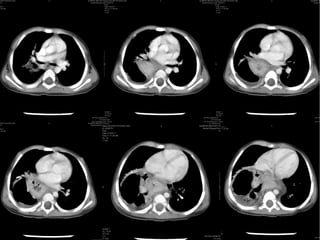
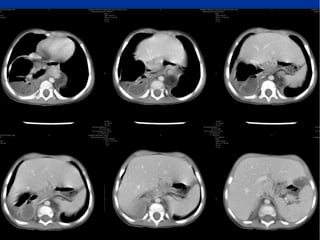
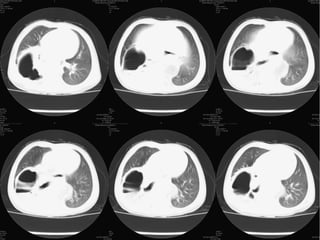
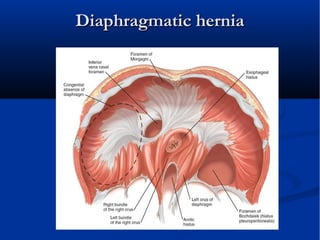

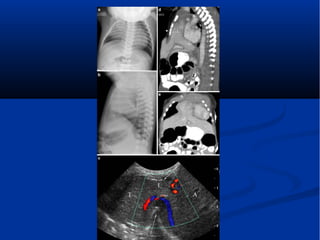
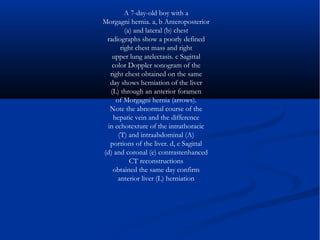
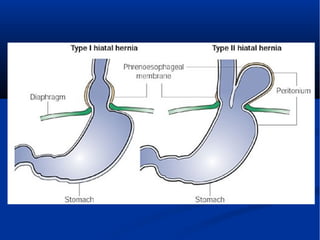




This report discusses imaging findings for a 19-month-old female patient being evaluated for a suspected lung abscess. The imaging shows a hiatal hernia where part of the stomach protrudes through the diaphragm. Specifically, it appears to be a paraesophageal type hernia where the gastroesophageal junction remains in the normal position but part of the stomach herniates into the chest. The report further describes the diagnosis and types of diaphragmatic and hiatal hernias seen on various imaging modalities like ultrasound, chest radiograph, CT and MRI.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



