Downloaded 42 times
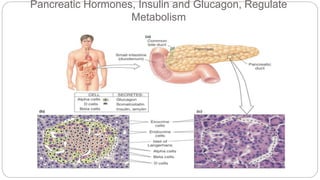
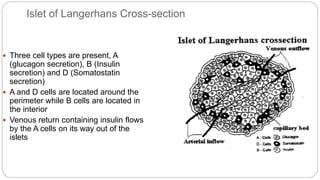
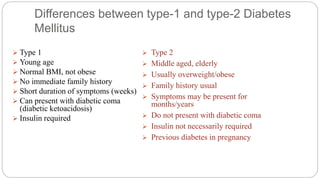


This document provides an overview of diabetes mellitus, including its classification into type 1 and type 2 diabetes. It defines each type, describing their pathophysiology, causes, signs and symptoms. Type 1 diabetes results from the body's immune system attacking insulin-producing beta cells in the pancreas. Type 2 involves insulin resistance and reduced insulin secretion. Diagnostic tests and treatment options are also reviewed, along with pancreatic anatomy and the role of insulin in regulating blood sugar levels. Complications of diabetes and collaborative care approaches are briefly mentioned.















![Diabetic ketoacidosis [DK]](https://cdn.slidesharecdn.com/ss_thumbnails/diabeticketoacidosis-200612175046-thumbnail.jpg?width=640&height=640&fit=bounds)














































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




